

Clinical and Morphologic Characteristics of Extracellular Signal-Regulated Kinase Inhibitor-Associated Retinopathy
- PMID: 34102344
- PMCID: PMC10977084
- DOI: 10.1016/j.oret.2021.06.001
Clinical and Morphologic Characteristics of Extracellular Signal-Regulated Kinase Inhibitor-Associated Retinopathy
Abstract
Purpose: To investigate clinical and morphologic characteristics of serous retinal disturbances in patients taking extracellular signal-regulated kinase (ERK) inhibitors.
Design: Single-center retrospective study of prospectively collected data.
Participants: Of 61 patients receiving ERK inhibitors for treatment of metastatic cancer, this study included 40 eyes of 20 patients with evidence of retinopathy confirmed by OCT.
Methods: Clinical examination, fundus photography, and OCT were used to evaluate ERK inhibitor retinopathy. The morphologic features, distribution, and location of fluid foci were evaluated serially. Visual acuity (VA) and choroidal thickness measurements were compared at baseline, fluid accumulation, and resolution.
Main outcome measures: Characteristics of treatment-emergent choroid and retinal OCT abnormalities as compared with baseline OCT findings and the impact of toxicity on VA.
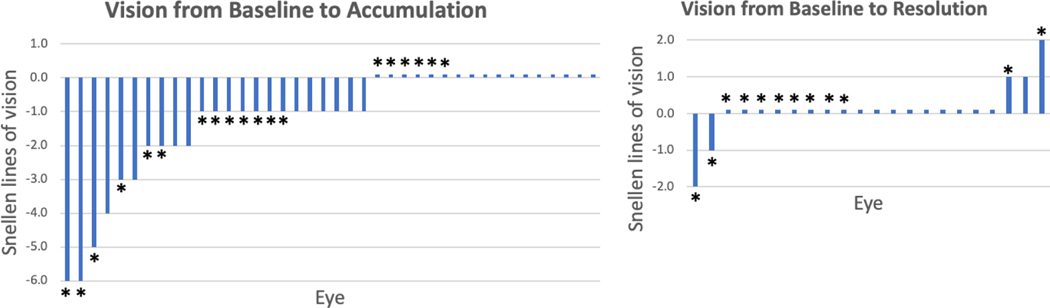
Results: Of 20 patients with retinopathy, most showed fluid foci that were bilateral (100%), multifocal in each eye (75%), and with at least 1 focus involving the fovea (95%). All subretinal fluid foci occurred between the interdigitation zone and an intact retinal pigment epithelium. No statistical difference was found in choroidal thickness at fluid accumulation and resolution compared with baseline. Forty-five percent of eyes showed evidence of concomitant intraretinal edema localized to the outer nuclear layer. At the time of fluid accumulation, 57.5% eyes showed a decline in VA (mainly by 1-2 lines from baseline). For all eyes with follow-up, the subretinal fluid and intraretinal edema were reversible and resolved without medical intervention, and best-corrected VA at fluid resolution was not statistically different from baseline. Concomitant intraretinal fluid was not associated with worsening of VA. No patient discontinued or decreased drug dose because of retinopathy.
Conclusions: This study showed that ERK inhibitors may cause subretinal fluid foci with unique clinical and morphologic characteristics. The observed foci were similar to mitogen-activated protein kinase kinase (MEK) inhibitor-associated retinopathy and distinct from central serous chorioretinopathy. However, unlike with MEK inhibitors, an increased occurrence of concomitant intraretinal fluid without significant additive visual impact seems to occur with ERK inhibitors. In this series, ERK inhibitors did not cause irreversible loss of vision or serious eye damage; retinopathy was self-limited and did not require medical intervention.
Keywords: Central serous chorioretinopathy; ERK inhibitor; MEK inhibitor; Retina; Subretinal fluid.
Copyright © 2021 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
COI: JHF- none, DHL-none, JC-none, JJH: has received research support from Bristol Myers Squibb and consulting fees from Bristol Myers Squibb, Eli Lilly, Exelexis, Eisai, QED, CytomX, Adaptimmune, Zymeworks, Imvax, and Merck, EIL- discloses editorial support from Pfizer Inc, outside the submitted work. BTL- grants from BioMedValley Discoveries, grants from National Institutes of Health, during the conduct of the study; grants from Genentech Roche, grants and personal fees from Guardant Health, grants and personal fees from Hengrui Therapeutics, grants from Lilly, grants from AstraZeneca, grants from Daiichi Sankyo, grants from Illumina, grants from GRAIL, grants and non-financial support from MORE Health, non-financial support from Resolution Bioscience, non-financial support from Jiangsu Hengrui Medicine, grants from Boehringer Ingelheim, grants from Bolt Biotherapeutics, grants from Amgen, outside the submitted work; In addition, Dr. Li has a patent US62/685,057 issued, and a patent US62/514,661 issued., IG- grants from Novartis, during the conduct of the study; grants and personal fees from Mirati Therapeutics, grants and personal fees from Janssen, personal fees from Basilea Therapeutica, grants from Bayer, grants from DeBioPharm, grants from Seagen, Inc, outside the submitted work, AD-grants from National Institutes of Health/National Cancer Institute, during the conduct of the study; personal fees from Ignyta/Genentech/Roche, personal fees from Loxo/Bayer/Lilly, personal fees from Takeda/Ariad/Millenium, personal fees from TP Therapeutics, personal fees from AstraZeneca, personal fees from Blueprint Medicines, personal fees from Helsinn, personal fees from Beigene, personal fees from BergenBio, personal fees from Hengrui Therapeutics, personal fees from Exelixis, personal fees from Tyra Biosciences, personal fees from Verastem, personal fees from MORE Health, personal fees from Abbvie, personal fees from 14ner/Elevation Oncology, personal fees from Remedica Ltd., personal fees from ArcherDX, personal fees from Monopteros, personal fees from Novartis, personal fees from EMD Serono, personal fees from Melendi, personal fees from Repare RX, personal fees from Pfizer, personal fees from Liberum, outside the submitted work; and Associated research paid to the institution from Pfizer, Exelixis, GlaxoSmithKline, Teva, Taiho, PharmaMar; research from Foundation Medicine; royalties from Wolters Kluwer; other support from Merck, Puma, Merus, Boehringer Ingelheim;and CME honoraria from Medscape, OncLive, PeerVoice, Physicians Education Resources, Targeted Oncology, Research to Practice, Axis,Peerview Institute, Paradigm Medical Communications, WebMD, MJH Life Sciences,Med Learning, Imedex,Answers in CME, Medscape, Clinical Care Options., AS- reports Funding to her institution for Clinical Trials: Merus Recipient, Kura Oncology Recipient, Surface Oncology Recipient, AstraZeneca Recipient, Lilly Recipient, Northern Biologics Recipient, Pfizer Recipient, Black Diamond Therapeutics Recipient, BeiGene Recipient, Relay Therapeutics Recipient, DHA-none
Figures




Comment in
-
Alphabet Soup: Clinical Pearls for the Retina Specialist-Ocular Toxicity of Advanced Antineoplastic Agents in Systemic Cancer Care.Ophthalmol Retina. 2021 Dec;5(12):1181-1186. doi: 10.1016/j.oret.2021.09.008. Ophthalmol Retina. 2021. PMID: 34872707
References
-
- Turner MC, Rossfeld K, Salama AKS, et al. Can binimetinib, encorafenib and masitinib be more efficacious than currently available mutation-based targeted therapies for melanoma treatment? Expert Opin Pharmacother 2017;18:487–495. - PubMed
-
- Dummer R, Schadendorf D, Ascierto PA, et al. Binimetinib versus dacarbazine in patients with advanced NRAS-mutant melanoma (NEMO): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 2017;18:435–445. - PubMed
-
- Suresh PS, Jairam RK, Chandrasekhar DV, et al. Prediction of Human Pharmacokinetics of Ulixertinib, a Novel ERK1/2 Inhibitor from Mice, Rats, and Dogs Pharmacokinetics. Eur J Drug Metab Pharmacokinet 2018;43:453–460. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
