

Effect of intra-arrest trans-nasal evaporative cooling in out-of-hospital cardiac arrest: a pooled individual participant data analysis
- PMID: 34103095
- PMCID: PMC8188685
- DOI: 10.1186/s13054-021-03583-9
Effect of intra-arrest trans-nasal evaporative cooling in out-of-hospital cardiac arrest: a pooled individual participant data analysis
Abstract
Background: Randomized trials have shown that trans-nasal evaporative cooling initiated during CPR (i.e. intra-arrest) effectively lower core body temperature in out-of-hospital cardiac arrest patients. However, these trials may have been underpowered to detect significant differences in neurologic outcome, especially in patients with initial shockable rhythm.
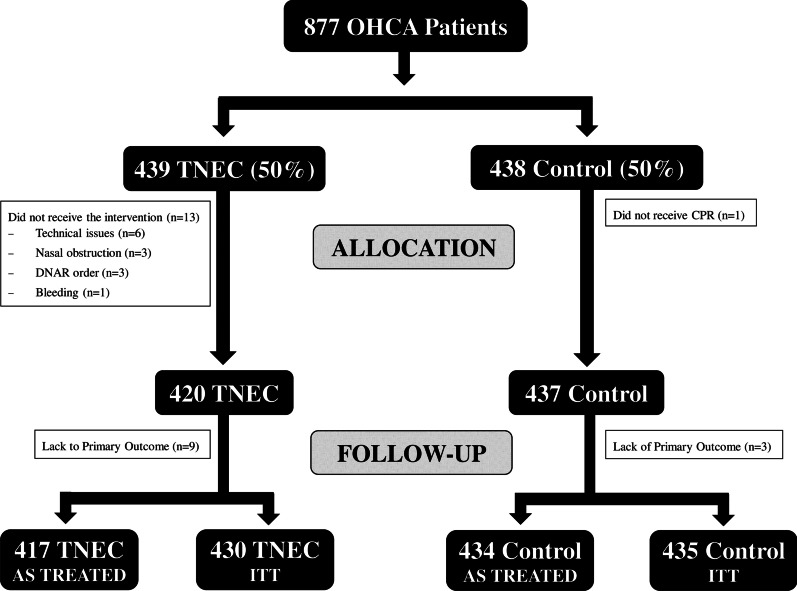
Methods: We conducted a post hoc pooled analysis of individual data from two randomized trials including 851 patients who eventually received the allocated intervention and with available outcome ("as-treated" analysis). Primary outcome was survival with favourable neurological outcome at hospital discharge (Cerebral Performance Category [CPC] of 1-2) according to the initial rhythm (shockable vs. non-shockable). Secondary outcomes included complete neurological recovery (CPC 1) at hospital discharge.
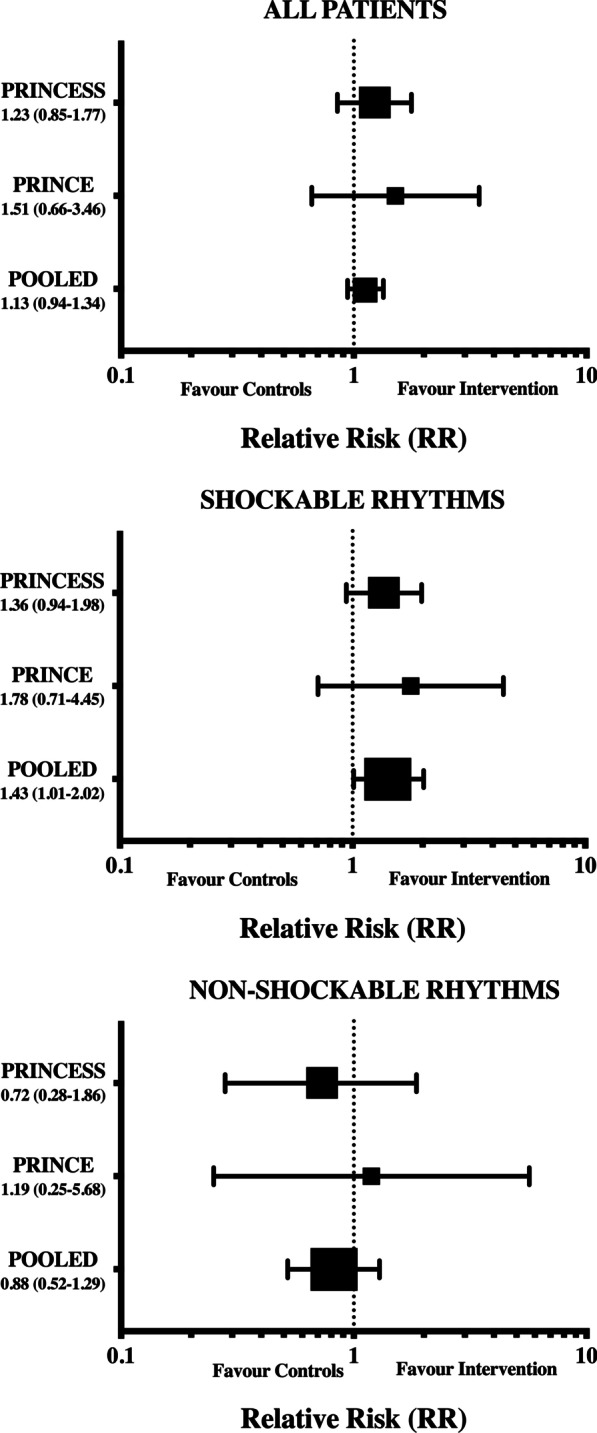
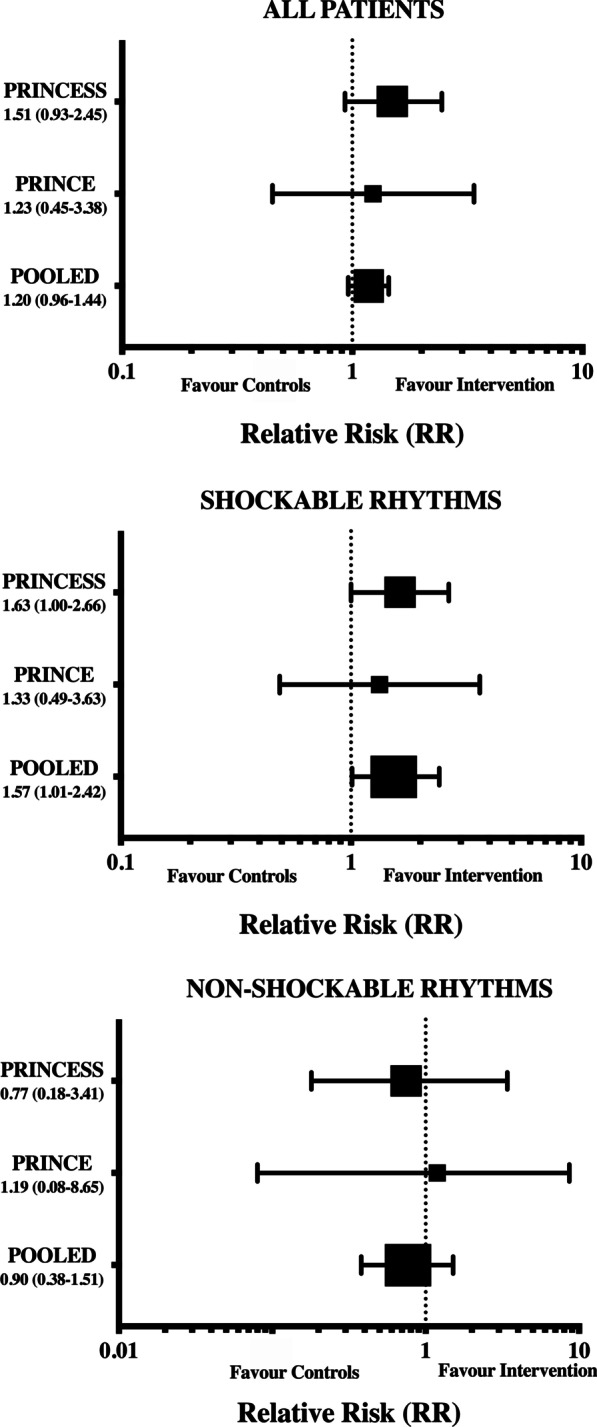
Results: Among the 325 patients with initial shockable rhythms, favourable neurological outcome was observed in 54/158 (34.2%) patients in the intervention and 40/167 (24.0%) in the control group (RR 1.43 [confidence intervals, CIs 1.01-2.02]). Complete neurological recovery was observed in 40/158 (25.3%) in the intervention and 27/167 (16.2%) in the control group (RR 1.57 [CIs 1.01-2.42]). Among the 526 patients with initial non-shockable rhythms, favourable neurological outcome was in 10/259 (3.8%) in the intervention and 13/267 (4.9%) in the control group (RR 0.88 [CIs 0.52-1.29]; p = 0.67); survival and complete neurological recovery were also similar between groups. No significant benefit was observed for the intervention in the entire population.
Conclusions: In this pooled analysis of individual data, intra-arrest cooling was associated with a significant increase in favourable neurological outcome in out-of-hospital cardiac arrest patients with initial shockable rhythms. Future studies are needed to confirm the potential benefits of this intervention in this subgroup of patients.
Keywords: Cardiac arrest; Hypothermia; Intra-arrest; Outcome; Randomized clinical trial.
Conflict of interest statement
Fabio Silvio TACCONE received lecture fees from BD. Fabio Silvio TACCONE also received lecture fees from ZOLL.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
