

Intravenous immunoglobulin treatment for mild Guillain-Barré syndrome: an international observational study
- PMID: 34103340
- PMCID: PMC8458059
- DOI: 10.1136/jnnp-2020-325815
Intravenous immunoglobulin treatment for mild Guillain-Barré syndrome: an international observational study
Abstract
Objective: To compare the disease course in patients with mild Guillain-Barré syndrome (GBS) who were treated with intravenous immunoglobulin (IVIg) or supportive care only.
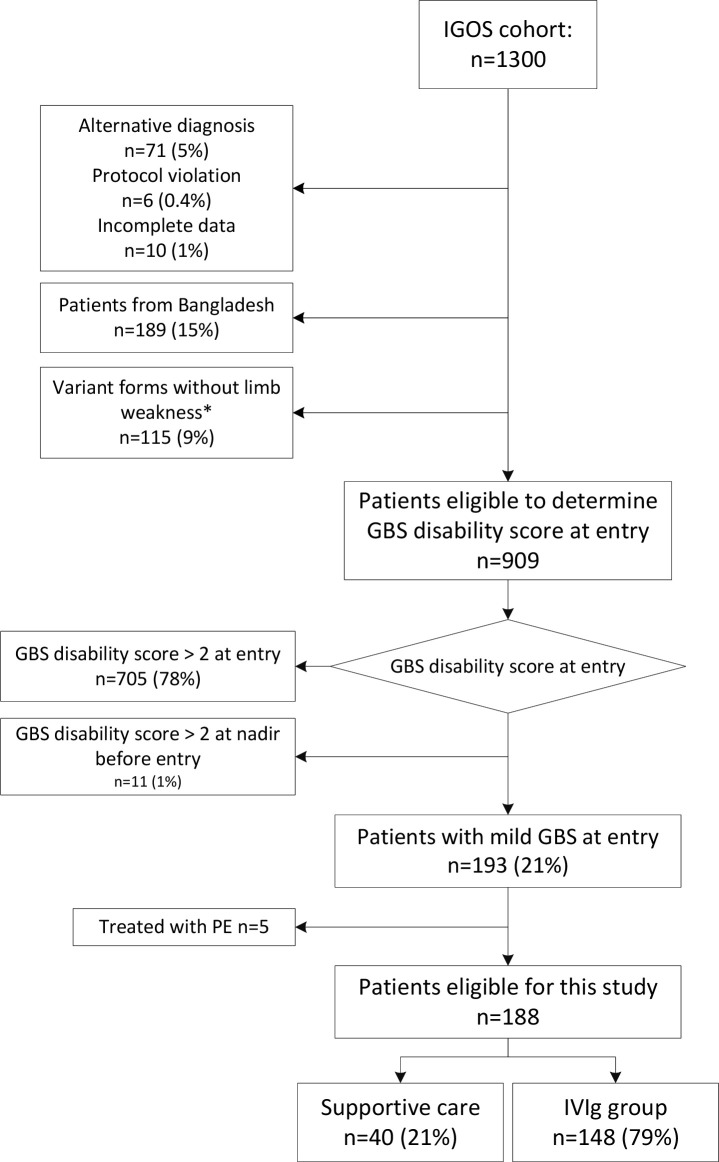
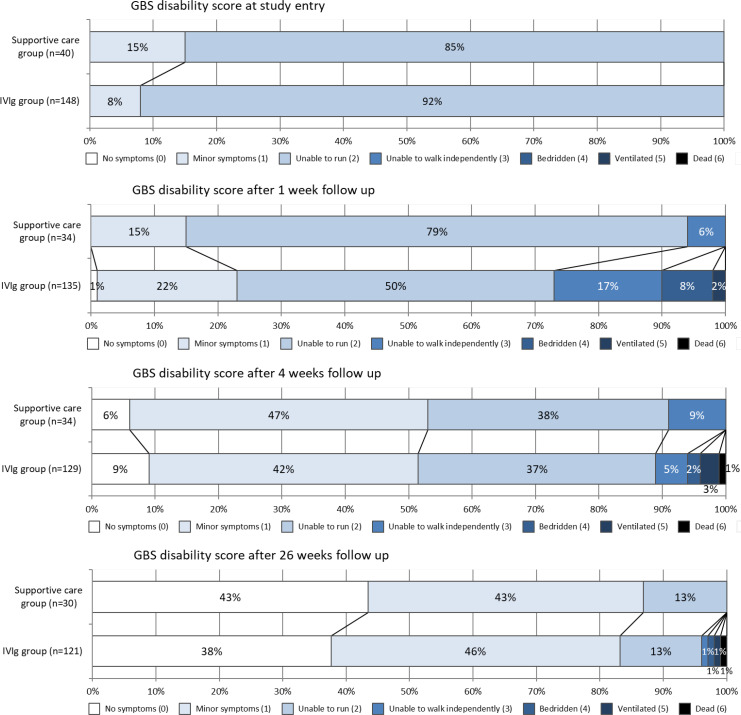
Methods: We selected patients from the prospective observational International GBS Outcome Study (IGOS) who were able to walk independently at study entry (mild GBS), treated with one IVIg course or supportive care. The primary endpoint was the GBS disability score four weeks after study entry, assessed by multivariable ordinal regression analysis.
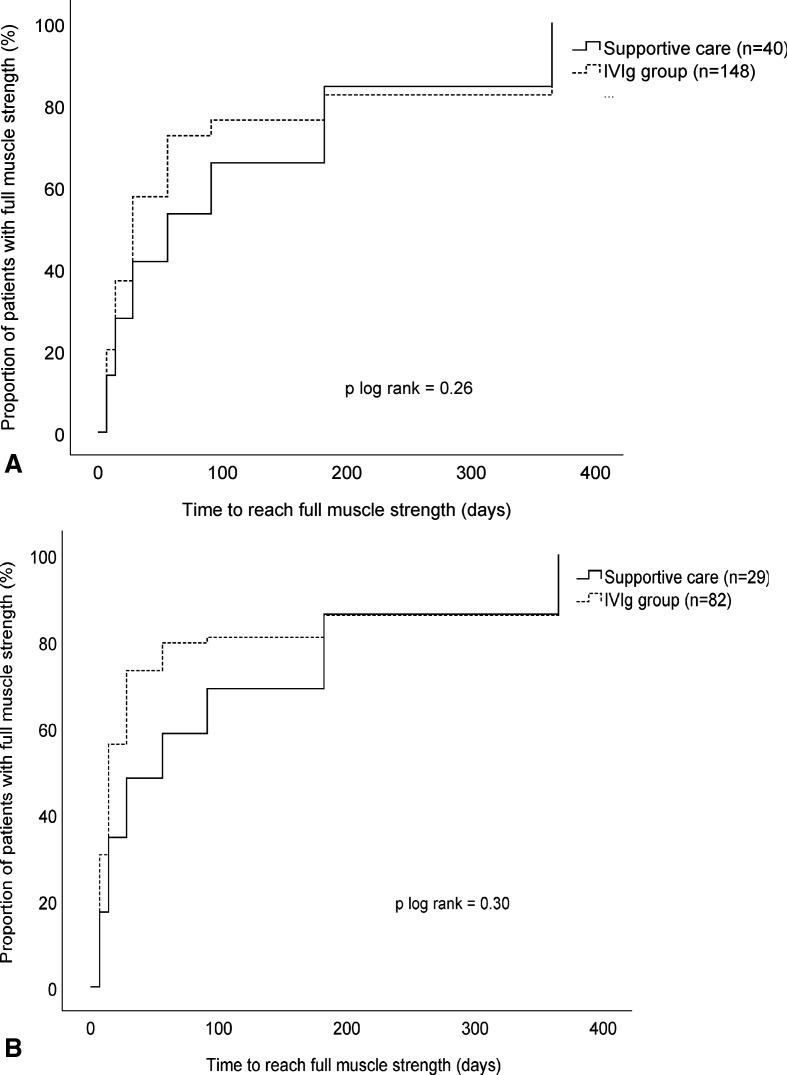
Results: Of 188 eligible patients, 148 (79%) were treated with IVIg and 40 (21%) with supportive care. The IVIg group was more disabled at baseline. IVIg treatment was not associated with lower GBS disability scores at 4 weeks (adjusted OR (aOR) 1.62, 95% CI 0.63 to 4.13). Nearly all secondary endpoints showed no benefit from IVIg, although the time to regain full muscle strength was shorter (28 vs 56 days, p=0.03) and reported pain at 26 weeks was lower (n=26/121, 22% vs n=12/30, 40%, p=0.04) in the IVIg treated patients. In the subanalysis with persistent mild GBS in the first 2 weeks, the aOR for a lower GBS disability score at 4 weeks was 2.32 (95% CI 0.76 to 7.13). At 1 year, 40% of all patients had residual symptoms.
Conclusion: In patients with mild GBS, one course of IVIg did not improve the overall disease course. The certainty of this conclusion is limited by confounding factors, selection bias and wide confidence limits. Residual symptoms were often present after one year, indicating the need for better treatments in mild GBS.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DRC is a consultant to Amgen, Annexon Biosciences, argenx SE, Biotest Pharmaceuticals, Boehringer Ingelheim, Cigna Health Management, CSL Behring, Grifols S.A., Neuropore, New Enterprise Associates, Octapharma AG, Passage Bio, Pfizer, Pharnext SAS, Polyneuron Pharmaceuticals, Sanofi-Aventis, Seattle Genetics and UCB Pharma. He is on Data Safety Monitoring Boards for Alnylam Pharmaceuticals, Anavex Life Sciences, PledPharma AB, Momenta Pharma, Hansa Medical AB and Mitsubishi Tanabe Pharma Corporation. He receives royalties for Technology Licensing from AstraZeneca Pharmaceuticals, LP, Genentech, Levicept, Seattle Genetics, Merrimack Pharmaceuticals, Disarm Therapeutics. RACH has consultancies with Hansa Biopharma, Immunic and Sanofi. PAvD has received honoraria for consulting, lectures and serving on steering committees from Octapharma, Kedrion, CSL Behring, Grifols and Hansa (all honoraria to departmental research fund) and received grants from the Prinses Beatrix Spierfonds, Sanquin Blood supply, Shire and Grifols for conducting clinical trials in GBS and CIDP. MPL is supported by the by the National Institute for Health Research University College London Hospitals Biomedical Research Centre. KCG has consulting agreements with Annexon, Argenx and UCB Pharma. BCJ has received funding for research projects from Prinses Beatrix Spierfonds, Horizon 2020, GBS-CIDP Foundation International, Grifols, CSL Behring, Annexon and Hansa Biopharma. He is on the Medical Advisory Board for the GBS-CIDP Foundation International, and a member of the Inflammatory Neuropathy Consortium.
Figures
Comment in
-
To treat or not to treat mild Guillain-Barré syndrome: limited evidence for but still none against.J Neurol Neurosurg Psychiatry. 2021 Oct;92(10):1027-1028. doi: 10.1136/jnnp-2021-326848. Epub 2021 Jun 8. J Neurol Neurosurg Psychiatry. 2021. PMID: 34103337 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical