

Degree of foot process effacement in patients with genetic focal segmental glomerulosclerosis: a single-center analysis and review of the literature
- PMID: 34103591
- PMCID: PMC8187362
- DOI: 10.1038/s41598-021-91520-9
Degree of foot process effacement in patients with genetic focal segmental glomerulosclerosis: a single-center analysis and review of the literature
Abstract
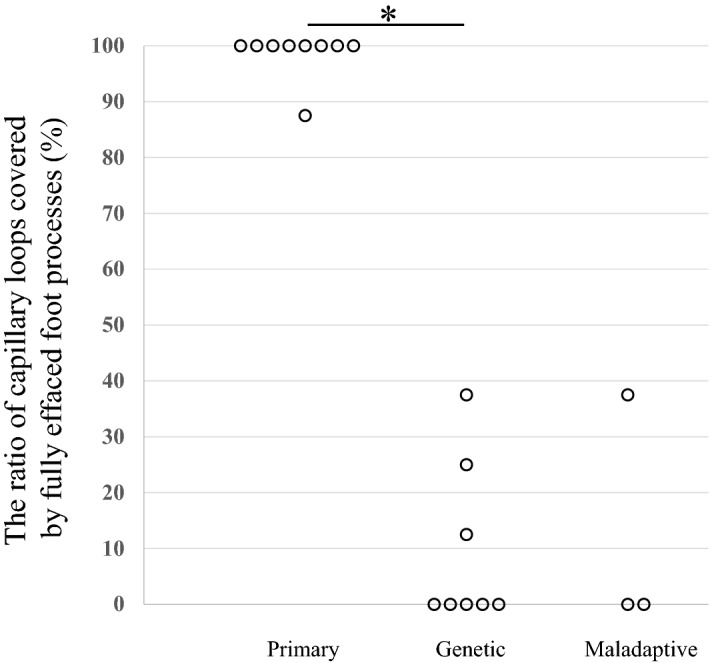
Determining the cause of focal segmental glomerulosclerosis (FSGS) has crucial implications for evaluating the risk of posttransplant recurrence. The degree of foot process effacement (FPE) on electron micrographs (EM) of native kidney biopsies can reportedly differentiate primary FSGS from secondary FSGS. However, no systematic evaluation of FPE in genetic FSGS has been performed. In this study, percentage of FPE and foot process width (FPW) in native kidney biopsies were analyzed in eight genetic FSGS patients and nine primary FSGS patients. All genetic FSGS patients showed segmental FPE up to 38% and FPW below 2000 nm, while all primary FSGS patients showed diffuse FPE above 88% and FPW above 3000 nm. We reviewed the literature which described the degree of FPE in genetic FSGS patients and identified 38 patients with a description of the degree of FPE. The degree of FPE in patients with mutations in the genes encoding proteins associated with slit diaphragm and cytoskeletal proteins was varied, while almost all patients with mutations in other FSGS genes showed segmental FPE. In conclusion, the present study suggests that the degree of FPE in native kidney biopsies may be useful for differentiating some genetic FSGS patients from primary FSGS patients.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
