

The protective effect of SARS-CoV-2 antibodies in Scottish healthcare workers
- PMID: 34104643
- PMCID: PMC8164012
- DOI: 10.1183/23120541.00080-2021
The protective effect of SARS-CoV-2 antibodies in Scottish healthcare workers
Abstract
Background: Healthcare workers (HCWs) are believed to be at increased risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. It is not known to what extent the natural production of antibodies to SARS-CoV-2 is protective against re-infection.
Methods: A prospective observational study of HCWs in Scotland (UK) from May to September 2020 was performed. The Siemens SARS-CoV-2 total antibody assay was used to establish seroprevalence in this cohort. Controls, matched for age and sex to the general local population, were studied for comparison. New infections (up to 2 December 2020) post antibody testing were recorded to determine whether the presence of SARS-CoV-2 antibodies protects against re-infection.
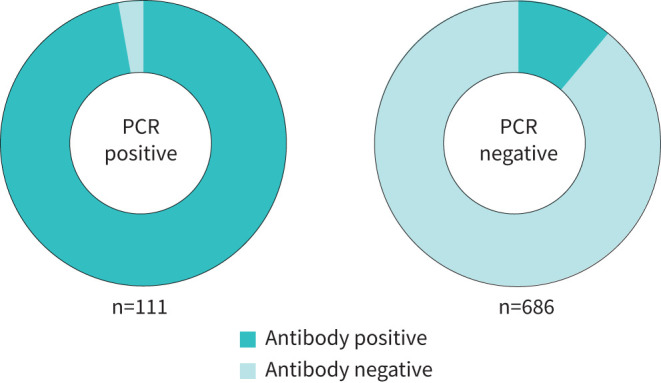
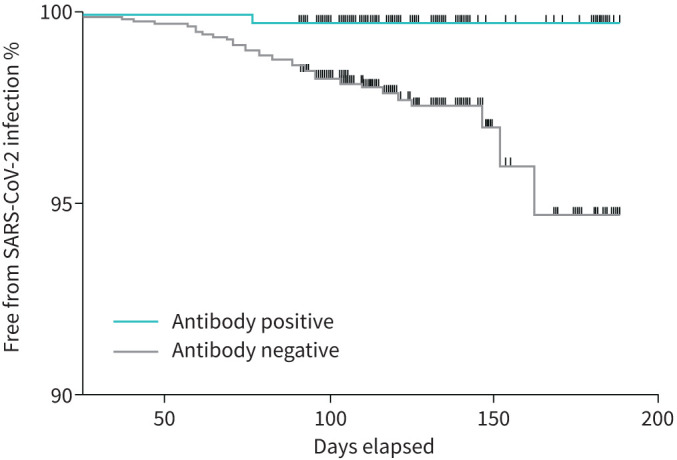
Results: A total of 2063 health and social care workers were recruited for this study. At enrolment, 300 HCWs had a positive antibody test (14.5%). 11 out of 231 control sera tested positive (4.8%). HCWs therefore had an increased likelihood of a positive test (OR 3.4, 95% CI 1.85-6.16; p<0.0001). Dentists were most likely to test positive. 97.3% of patients who had previously tested positive for SARS-CoV-2 by reverse transcriptase (RT)-PCR had positive antibodies. 18.7% had an asymptomatic infection. There were 38 new infections with SARS-CoV-2 in HCWs who were previously antibody negative, and one symptomatic RT-PCR-positive re-infection. The presence of antibodies was therefore associated with an 85% reduced risk of re-infection with SARS-CoV-2 (hazard ratio 0.15, 95% CI 0.06-0.35; p=0.026).
Conclusion: HCWs were three times more likely to test positive for SARS-CoV-2 than the general population. Almost all infected individuals developed an antibody response, which was 85% effective in protecting against re-infection with SARS-CoV-2.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: H. Abo-Leyah has nothing to disclose. Conflict of interest: S. Gallant has nothing to disclose. Conflict of interest: D. Cassidy has nothing to disclose. Conflict of interest: Y.H. Giam has nothing to disclose. Conflict of interest: J. Killick has nothing to disclose. Conflict of interest: B. Marshall has nothing to disclose. Conflict of interest: G. Hay has nothing to disclose. Conflict of interest: C. Snowdon has nothing to disclose. Conflict of interest: E.J. Hothersall has nothing to disclose. Conflict of interest: T. Pembridge has nothing to disclose. Conflict of interest: R. Strachan has nothing to disclose. Conflict of interest: N. Gallant has nothing to disclose. Conflict of interest: B.J. Parcell has nothing to disclose. Conflict of interest: J. George has nothing to disclose. Conflict of interest: E. Furrie has nothing to disclose. Conflict of interest: J.D. Chalmers reports grants and personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Insmed; personal fees from Chiesi, Novartis and Zambon; and grants from Gilead Sciences, all outside the submitted work.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous