

Evolution of outcomes for patients hospitalised during the first 9 months of the SARS-CoV-2 pandemic in France: A retrospective national surveillance data analysis
- PMID: 34104903
- PMCID: PMC7981225
- DOI: 10.1016/j.lanepe.2021.100087
Evolution of outcomes for patients hospitalised during the first 9 months of the SARS-CoV-2 pandemic in France: A retrospective national surveillance data analysis
Abstract
Background: As SARS-CoV-2 continues to spread, a thorough characterisation of healthcare needs and patient outcomes, and how they have changed over time, is essential to inform planning.
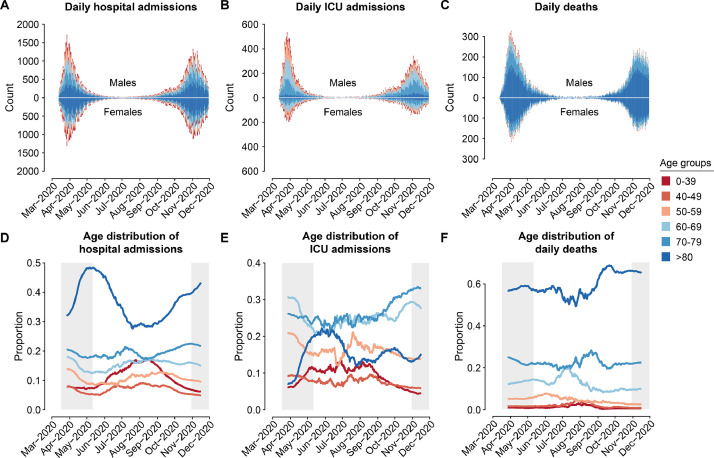
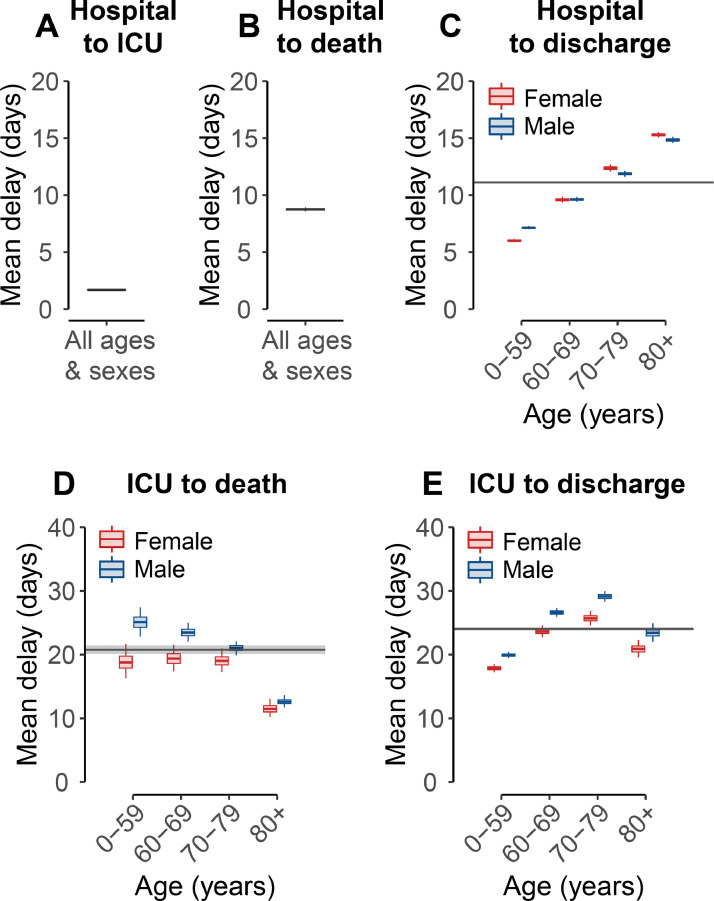
Methods: We developed a probabilistic framework to analyse detailed patient trajectories from 198,846 hospitalisations in France during the first nine months of the pandemic. Our model accounts for the varying age- and sex- distribution of patients, and explore changes in outcome probabilities as well as length of stay.
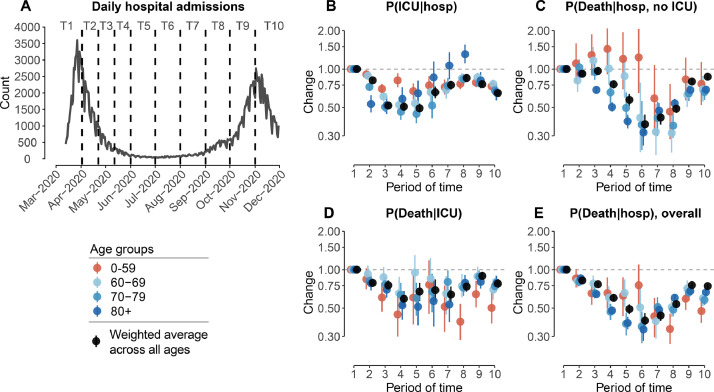
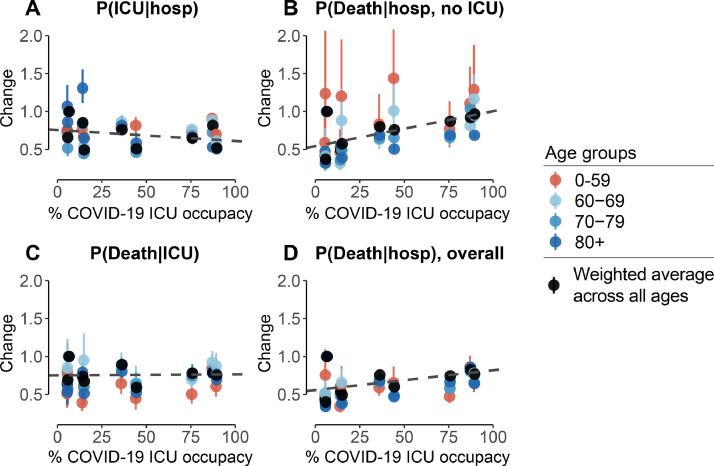
Findings: We found that there were marked changes in the age and sex of hospitalisations over the study period. In particular, the proportion of hospitalised individuals that were >80y varied between 27% and 48% over the course of the epidemic, and was lowest during the inter-peak period. The probability of hospitalised patients entering ICU dropped from 0·25 (0·24-0·26) to 0·13 (0·12-0·14) over the four first months as case numbers fell, before rising to 0·19 (0·19-0·20) during the second wave. The probability of death followed a similar trajectory, falling from 0·25 (0·24-0·26) to 0·10 (0·09-0·11) after the first wave before increasing again during the second wave to 0·19 (0·18-0·19). Overall, we find both the probability of death and the probability of entering ICU were significantly correlated with COVID-19 ICU occupancy.
Interpretation: There are large scale trends in patients outcomes by age, sex and over time. These need to be considered in ongoing healthcare planning efforts.
Funding: INCEPTION.
© 2021 The Authors.
Conflict of interest statement
N.L, J.P., N.H., N.C., L.B., P.-Y.B., Y.Y., F.C. and S.C. have nothing to disclose. YY has been a board member receiving consultancy fees from ABBVIE, BMS, Gilead, MSD, J&J, Pfizer, and ViiV Healthcare, however, all these activities have been stopped in the 3 past years. H.S. reports personal fees from AstraZeneca Data Safety Monitoring Board, outside the submitted work.
Figures

References
-
- Flaxman S., Mishra S., Gandy A., Unwin H.J.T., Mellan T.A., Coupland H. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature. 2020;584(7820):257–261. - PubMed
-
- Massonnaud C., Roux J., Crépey P. COVID-19: forecasting short term hospital needs in France. medRxiv. 2020 https://www.medrxiv.org/content/10.1101/2020.03.16.20036939v1.abstract Available from: - DOI
-
- Andronico A., Kiem C.T., Paireau J., Succo T., Bosetti P., Lefrancq N. Evaluating the impact of curfews and other measures on SARS-CoV-2 transmission in French Guiana. medRxiv. 2020 https://www.medrxiv.org/content/10.1101/2020.10.07.20208314v1.abstract Available from. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
