

Validation of High-Sensitivity Severe Acute Respiratory Syndrome Coronavirus 2 Testing for Stool-Toward the New Normal for Fecal Microbiota Transplantation
- PMID: 34106090
- PMCID: PMC8189625
- DOI: 10.14309/ctg.0000000000000363
Validation of High-Sensitivity Severe Acute Respiratory Syndrome Coronavirus 2 Testing for Stool-Toward the New Normal for Fecal Microbiota Transplantation
Abstract
Introduction: Mounting evidence demonstrates potential for fecal-oral transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The US Food and Drug Administration now requires SARS-CoV-2 testing of potential feces donors before the use of stool manufactured for fecal microbiota transplantation. We sought to develop and validate a high-sensitivity SARS-CoV-2 reverse transcriptase polymerase chain reaction (RT-PCR) procedure for testing stool specimens.
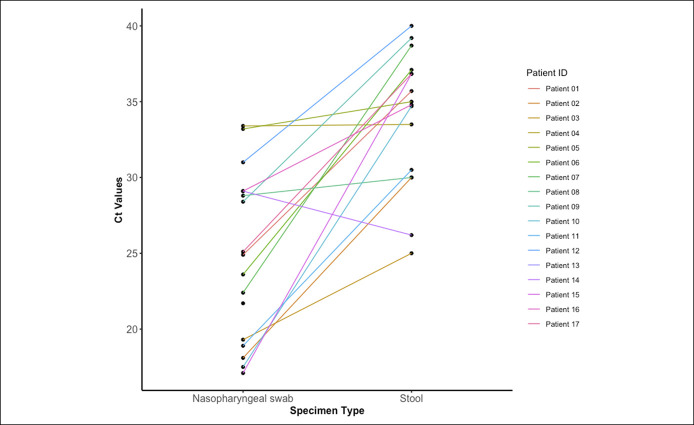
Methods: A modified extraction method was used with an RT-PCR assay adapted from the Centers for Disease Control and Prevention PCR protocol for respiratory specimens. Contrived specimens were created using pre-COVID-19 banked stool specimens and spiking in known concentrations of SARS-CoV-2-specific nucleic acid. The highest transcript concentration at which 2/2 or 1/2 SARS-CoV-2 targets were detected in 9/10 replicates was defined as the dual-target limit and single-target limit of detection, respectively. The clinical performance of the assay was evaluated with stool samples collected from 17 nasopharyngeal swab RT-PCR-positive patients and 14 nasopharyngeal RT-PCR-negative patients.
Results: The dual-target and single-target limit of detection were 56 copies/μL and 3 copies/μL, respectively. SARS-CoV-2 was detected at concentrations as low as 0.6 copies/μL. Clinical stool samples from known COVID-19-positive patients demonstrated the detection of SARS-CoV-2 in stool up to 29 days from symptom onset with a high agreement with nasopharyngeal swab tests (kappa statistic of 0.95, P value < 0.001).
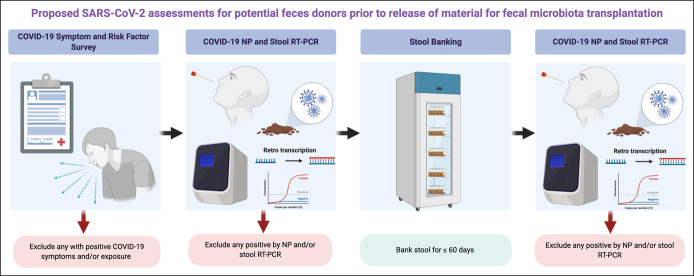
Discussion: The described RT-PCR test is a sensitive and flexible approach for the detection of SARS-CoV-2 in stool specimens. We propose an integrated screening approach that incorporates this stool test to support continuation of fecal microbiota transplantation programs.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
References
-
- Wölfel R, Corman VM, Guggemos W, et al. . Virological assessment of hospitalized patients with COVID-2019. Nature 2020;581:465–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
