

Estimated Cardiorespiratory Hospitalizations Attributable to Influenza and Respiratory Syncytial Virus Among Long-term Care Facility Residents
- PMID: 34106266
- PMCID: PMC8190624
- DOI: 10.1001/jamanetworkopen.2021.11806
Estimated Cardiorespiratory Hospitalizations Attributable to Influenza and Respiratory Syncytial Virus Among Long-term Care Facility Residents
Abstract
Importance: Older adults residing in long-term care facilities (LTCFs) are at a high risk of being infected with respiratory viruses, such as influenza and respiratory syncytial virus (RSV). Although these infections commonly have many cardiorespiratory sequelae, the national burden of influenza- and RSV-attributable cardiorespiratory events remains unknown for the multimorbid and vulnerable LTCF population.
Objective: To estimate the incidence of cardiorespiratory hospitalizations that were attributable to influenza and RSV among LTCF residents and to quantify the economic burden of these hospitalizations on the US health care system by estimating their associated cost and length of stay.
Design, setting, and participants: This retrospective cohort study used national Medicare Provider Analysis and Review inpatient claims and Minimum Data Set clinical assessments for 6 respiratory seasons (2011-2017). Long-stay residents of LTCFs were identified as those living in the facility for at least 100 days (index date), aged 65 years or older, and with 6 months of continuous enrollment in Medicare Part A were included. Follow-up occurred from the resident's index date until the first hospitalization, discharge from the LTCF, disenrollment from Medicare, death, or the end of the study. Residents could re-enter the sample; thus, long-stay episodes of care were identified. Data analysis was performed between January 1 and September 30, 2020.
Exposures: Seasonal circulating pandemic 2009 influenza A(H1N1), human influenza A(H3N2), influenza B, and RSV.
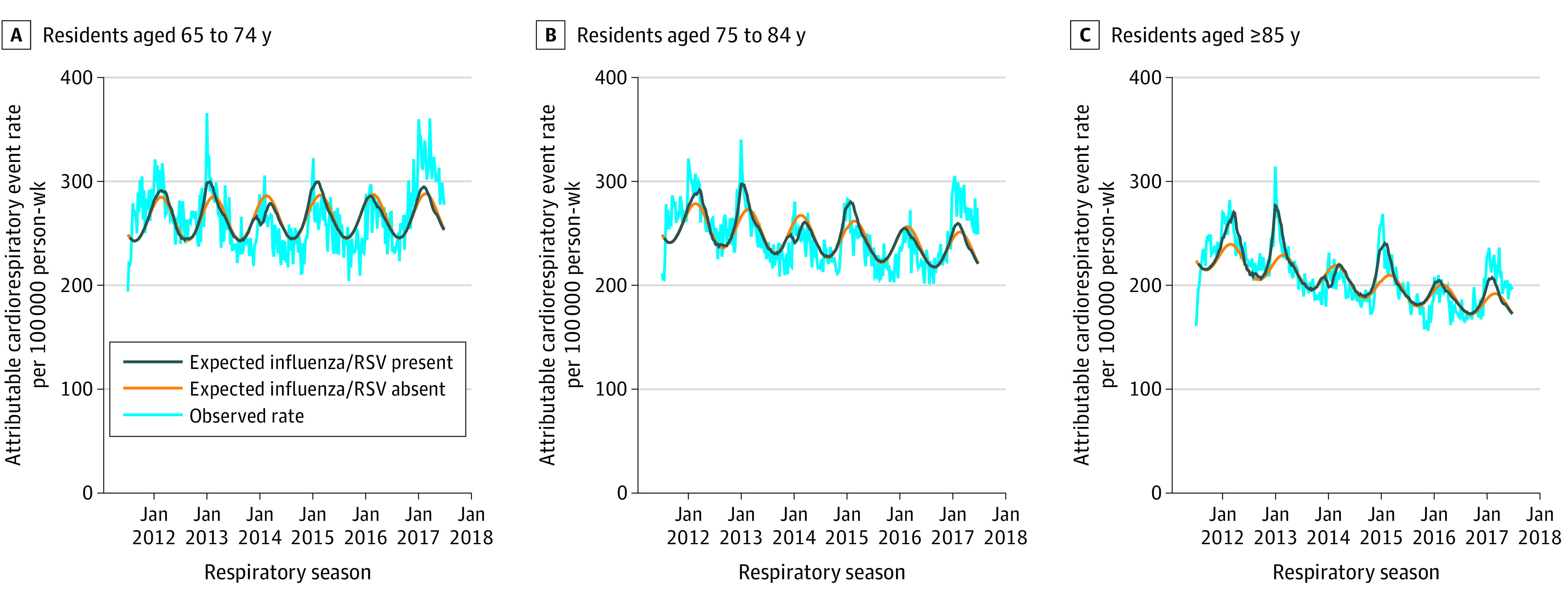
Main outcomes and measures: Cardiorespiratory hospitalizations (eg, asthma exacerbation, heart failure) were identified using primary diagnosis codes. Influenza- and RSV-attributable cardiorespiratory events were estimated using a negative binomial regression model adjusted for weekly circulating influenza and RSV testing data. Length of stay and costs of influenza- and RSV-attributable events were then estimated.
Results: The study population comprised 2 909 106 LTCF residents with 3 138 962 long-stay episodes and 5 079 872 person-years of follow-up. Overall, 10 939 (95% CI, 9413-12 464) influenza- and RSV-attributable cardiorespiratory events occurred, with an incidence of 215 (95% CI, 185-245) events per 100 000 person-years. The cost of influenza- and RSV-attributable cardiorespiratory events was $91 055 393 (95% CI, $77 885 316-$104 225 470), and the length of stay was 56 858 (95% CI, 48 757-64 968) days.
Conclusions and relevance: This study found that many cardiorespiratory hospitalizations among LTCF residents in the US were attributable to seasonal influenza and RSV. To minimize the burden these events place on the health care system and residents of LTCFs and to prevent virus transmission, additional preventive measures should be implemented.
Conflict of interest statement
Figures
References
-
- Rolfes MA, Foppa IM, Garg S, et al. . 2015-2016 Estimated influenza illnesses, medical visits, hospitalizations, and deaths averted by vaccination in the United States. Accessed April 3, 2021. https://www.cdc.gov/flu/about/disease/2015-16.htm
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
