

How the coronavirus disease 2019 pandemic changed the patterns of healthcare utilization by geriatric patients and the crowding: a call to action for effective solutions to the access block
- PMID: 34106397
- PMCID: PMC8188157
- DOI: 10.1007/s11739-021-02732-w
How the coronavirus disease 2019 pandemic changed the patterns of healthcare utilization by geriatric patients and the crowding: a call to action for effective solutions to the access block
Abstract
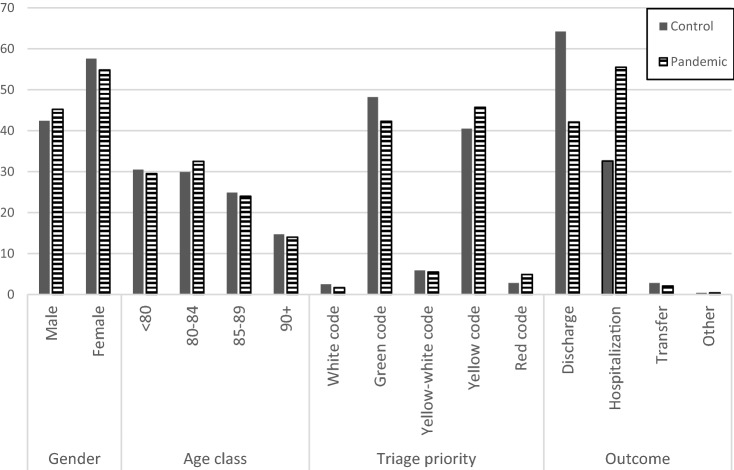
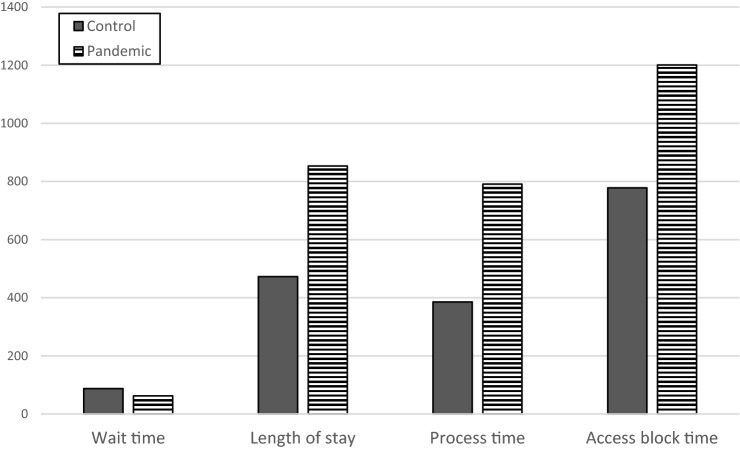
The geriatric population constitutes a large slice of the population of Western countries and a class of fragile patients, with greater deaths due to COVID-19. The patterns of healthcare utilization change during pandemic disease outbreaks. Identifying the patterns of changes of this particular fragile subpopulation is important for future preparedness and response. Overcrowding in the emergency department (ED) can occur because of the volume of patients waiting to be seen, delays in patient assessment or treatment in the ED, or impediments to leaving the ED once the treatment has been completed. Overcrowding has become a serious and growing issue globally, which represents a serious impediment to healthcare utilization. To estimate the rate of ED visits attributable to the outbreak and guide the planning of strategies for managing ED access or after the outbreak of transmittable respiratory diseases. This observational study was based on a retrospective review of the epidemiological and clinical records of patients aged > 75 years who visited the Foundation IRCCS Policlinic San Matteo during the first wave of COVID-19 outbreak (February 21 to May 1, 2020; pandemic group). The analysis methods included estimation of the changes in the epidemiological and clinical data from the annual baseline data after the start of the COVID-19 pandemic. Outcome measures and analysis: Primary objective is the evaluation of ED admission rate change and ED overcrowding. Secondary objectives are the evaluation of modes of ED access by reason and triage code, access types, clinical outcomes (such as admission and mortality rates). During the pandemic, ED crowding increased dramatically, although the overall number of patients decreased, in the face of a percentage increase in those with high-acuity conditions, because of changes in patient management that have prolonged length of stay (LOS) and increased rates of access block. Overcrowding during the COVID-19 pandemic can be attributed to the Access Block. Access Block solutions are hence required to prevent a recurrence of crowding to any new viral wave or new epidemic in the future.
Keywords: Access block; Coronavirus disease; Crowding; Emergency care utilization; Emergency department; Exit block; Pandemic.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- World Health Organization (WHO) (2020) Coronavirus disease 2019 (COVID-19), Situation Report-65. data as reported by ational authorities by 10:00 CET 25 March 2020. https://www.who.int/docs/default-source/coronaviruse/situationreports/20.... Accessed 25 Mar 2020
-
- Asperges E, Novati S, Muzzi A, Biscarini S, Sciarra M, Lupi M, Sambo M, Gallazzi I, Peverini M, Lago P, Mojoli F. Rapid response to COVID-19 outbreak in Northern Italy: how to convert a classic infectious disease ward into a COVID-19 response centre. J Hosp Infect. 2020;105(3):477–479. doi: 10.1016/j.jhin.2020.03.020. - DOI - PMC - PubMed
-
- Satia I, Cusack R, Greene JM, O’Byrne PM, Killian KJ, et al. Prevalence and contribution of respiratory viruses in the community to rates of emergency department visits and hospitalizations with respiratory tract infections, chronic obstructive pulmonary disease and asthma. PLoS ONE. 2020;15(2):e0228544. doi: 10.1371/journal.pone.0228544. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
