

Treatment outcomes in HIV infected patients older than 50 years attending an HIV clinic in Harare, Zimbabwe: A cohort study
- PMID: 34106989
- PMCID: PMC8189507
- DOI: 10.1371/journal.pone.0253000
Treatment outcomes in HIV infected patients older than 50 years attending an HIV clinic in Harare, Zimbabwe: A cohort study
Abstract
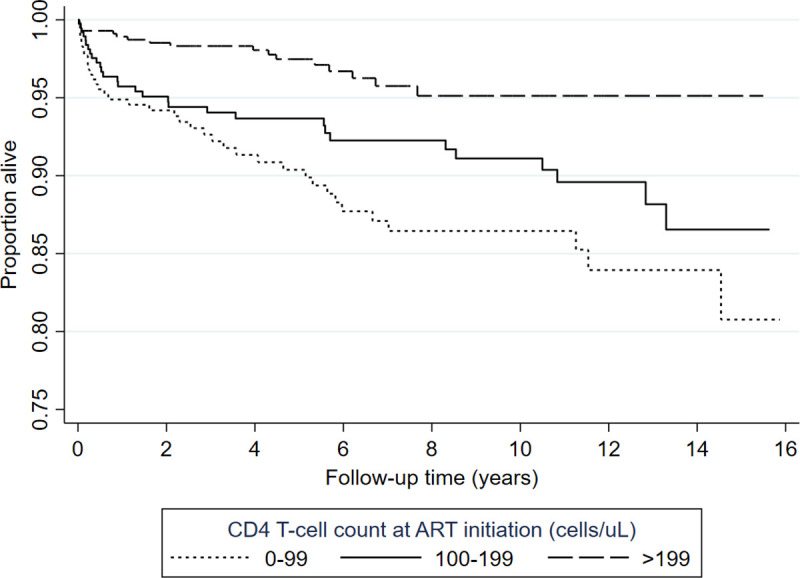
There is a growing number of older people living with HIV (OPLHIV). While a significant proportion of this population are adults growing into old age with HIV, there are also new infections among OPLHIV. There is a lack of data describing the outcomes of OPLHIV who commenced antiretroviral therapy (ART) after the age of 50 years in sub-Saharan Africa. We conducted a cohort study of patients who enrolled in care at Newlands Clinic in Harare, Zimbabwe, at ages ≥50 years between February 2004 and March 2020. We examined demographic characteristics, attrition, viral suppression, immunological and clinical outcomes. Specifically, we described prevalent and incident HIV-related communicable and non-communicable comorbidities. We calculated frequencies, medians, interquartile ranges (IQR), and proportions; and used Cox proportional hazards models to identify risk factors associated with death. We included 420 (57% female) who commenced ART and were followed up for a median of 5.6 years (IQR 2.4-9.9). Most of the men were married (n = 152/179, 85%) whereas women were mostly widowed (n = 125/241, 51.9%). Forty per cent (n = 167) had WHO stage 3 or 4 conditions at ART baseline. Hypertension prevalence was 15% (n = 61) at baseline, and a further 27% (n = 112) had incident hypertension during follow-up. During follow-up, 300 (71%) were retained in care, 88 (21%) died, 17 (4%) were lost to follow-up, and 15 (4%) were transferred out. Of those in care, 283 (94%) had viral loads <50 copies/ml, and 10 had viral loads >1000 copies/ml. Seven patients (1.7%) were switched to second line ART during follow-up and none were switched to third-line. Higher baseline CD4 T-cell counts were protective against mortality (p = 0.001) while male sex (aHR: 2.29, 95%CI: 1.21-4.33), being unmarried (aHR: 2.06, 95%CI: 1.13-3.78), and being unemployed (aHR: 2.01, 95%CI: 1.2-3.37) were independent independent risk factors of mortality. There was high retention in care and virologic suppression in this cohort of OPLHIV. Hypertension was a common comorbidity. Being unmarried or unemployed were significant predictors of mortality highlighting the importance of sociologic factors among OPLHIV, while better immune competence at ART commencement was protective against mortality.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- AIDSinfo | UNAIDS. [cited 5 Oct 2020]. Available: https://aidsinfo.unaids.org/
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
