

Adjunct Immune Globulin for Vaccine-Induced Immune Thrombotic Thrombocytopenia
- PMID: 34107198
- PMCID: PMC8362588
- DOI: 10.1056/NEJMoa2107051
Adjunct Immune Globulin for Vaccine-Induced Immune Thrombotic Thrombocytopenia
Abstract
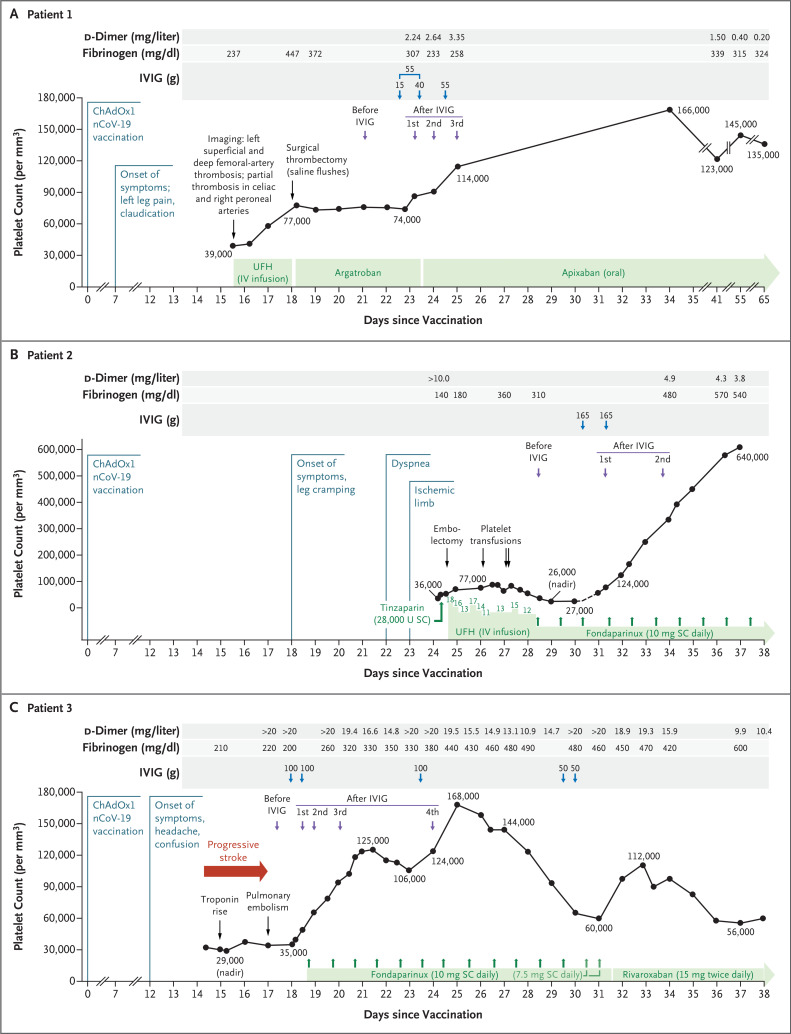
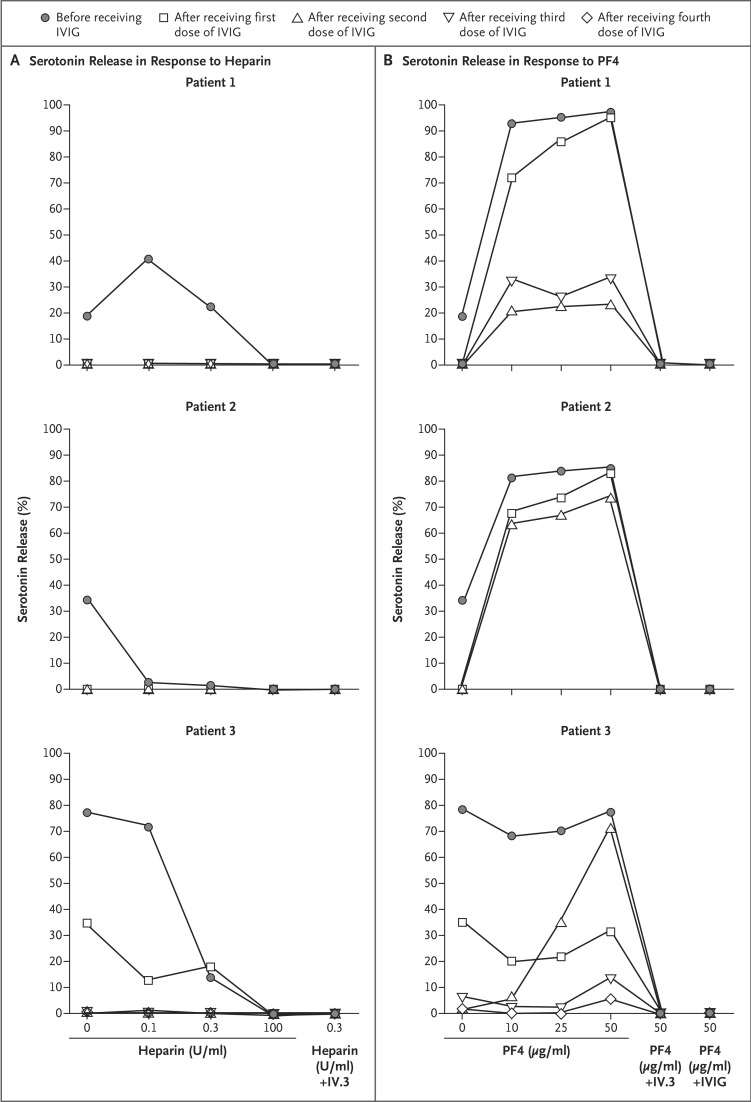
The use of high-dose intravenous immune globulin (IVIG) plus anticoagulation is recommended for the treatment of vaccine-induced immune thrombotic thrombocytopenia (VITT), a rare side effect of adenoviral vector vaccines against coronavirus disease 2019 (Covid-19). We describe the response to IVIG therapy in three of the first patients in whom VITT was identified in Canada after the receipt of the ChAdOx1 nCoV-19 vaccine. The patients were between the ages of 63 and 72 years; one was female. At the time of this report, Canada had restricted the use of the ChAdOx1 nCoV-19 vaccine to persons who were 55 years of age or older on the basis of reports that VITT had occurred primarily in younger persons. Two of the patients in our study presented with limb-artery thrombosis; the third had cerebral venous and arterial thrombosis. Variable patterns of serum-induced platelet activation were observed in response to heparin and platelet factor 4 (PF4), indicating the heterogeneity of the manifestations of VITT in serum. After the initiation of IVIG, reduced antibody-induced platelet activation in serum was seen in all three patients. (Funded by the Canadian Institutes of Health Research.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Thrombotische Thrombozytopenie nach Vektorimpfstoff: So wird therapiert.MMW Fortschr Med. 2022 Feb;164(2):28. doi: 10.1007/s15006-022-0747-9. MMW Fortschr Med. 2022. PMID: 35088323 Free PMC article. Review. German. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous