

Membranous nephropathy associated with multicentric Castleman's disease that was successfully treated with tocilizumab: a case report and review of the literature
- PMID: 34107915
- PMCID: PMC8191014
- DOI: 10.1186/s12882-021-02423-w
Membranous nephropathy associated with multicentric Castleman's disease that was successfully treated with tocilizumab: a case report and review of the literature
Abstract
Background: Multicentric Castleman's disease is a life-threatening disorder involving a systemic inflammatory response and multiple organ failure caused by the overproduction of interleukin-6. Although renal complications of Castleman's disease include AA amyloidosis, thrombotic microangiopathy, and membranoproliferative glomerulonephritis, membranous nephropathy is relatively rare. We experienced a case of secondary membranous nephropathy associated with Castleman's disease.
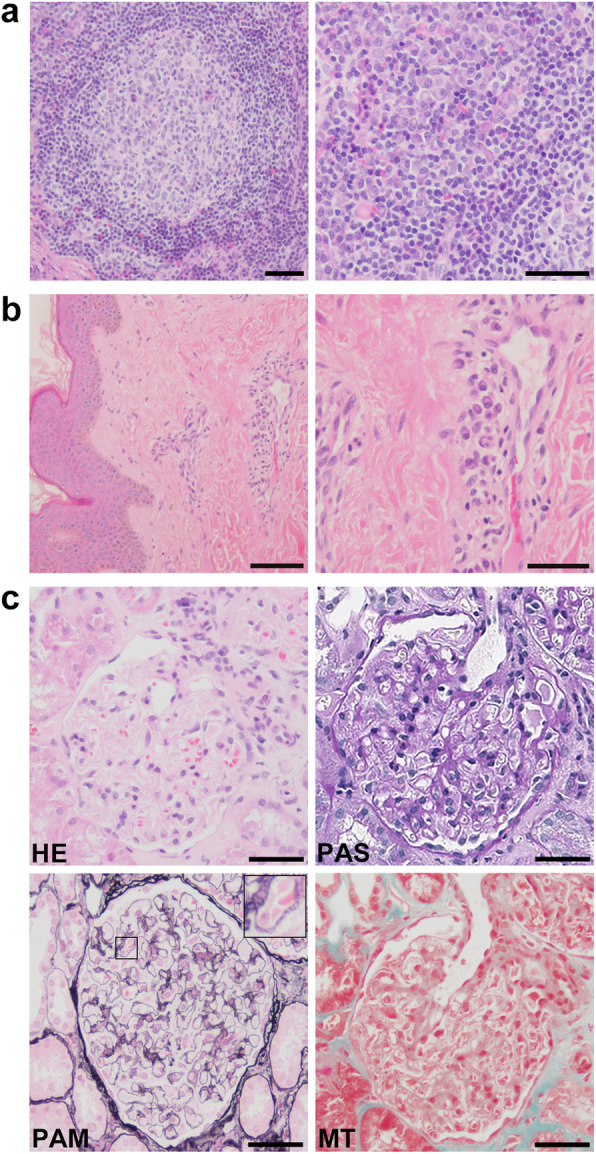
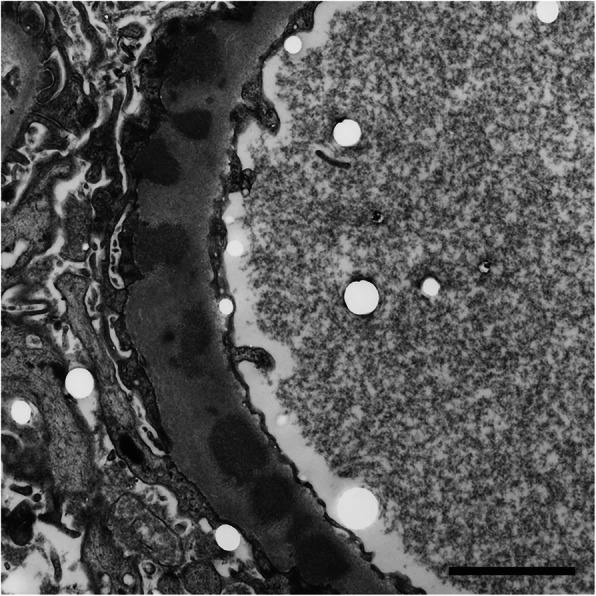
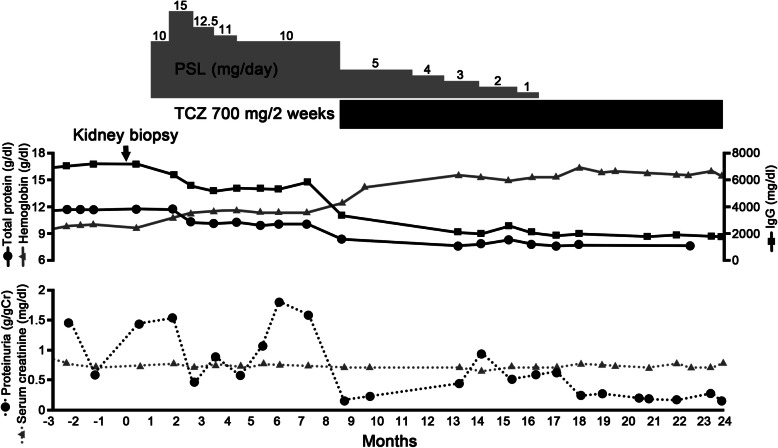
Case presentation: The patient was a 43-year-old Japanese man who had shown a high zinc sulfate value in turbidity test, polyclonal hypergammaglobulinemia, anemia, and proteinuria. A physical examination revealed diffuse lymphadenopathy, an enlarged spleen and papulae of the body trunk. A skin biopsy of a papule on the patient's back showed plasma cells in the perivascular area and he was diagnosed with multicentric Castleman's disease, plasma cell variant. Kidney biopsy showed the appearance of bubbling in the glomerular basement membranes in Periodic acid methenamine silver stain and electron microscopy revealed electron dense deposits within and outside the glomerular basement membranes. Since immunofluorescence study showed predominant granular deposition of IgG1 and IgG2, he was diagnosed with secondary membranous nephropathy associated with Castleman's disease. He was initially treated with prednisolone alone, however his biochemical abnormalities did not improve. After intravenous tocilizumab (700 mg every 2 weeks) was started, his C-reactive protein elevation, anemia, and polyclonal gammopathy improved. Furthermore, his urinary protein level declined from 1.58 g/gCr to 0.13 g/gCr. The prednisolone dose was gradually tapered, then discontinued. He has been stable without a recurrence of proteinuria for more than 6 months.
Conclusions: Tocilizumab might be a treatment option for secondary membranous nephropathy associated with Castleman's disease.
Keywords: Castleman’s disease - membranous nephropathy; Proteinuria - tocilizumab.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials
