

Importance of patient bed pathways and length of stay differences in predicting COVID-19 hospital bed occupancy in England
- PMID: 34107928
- PMCID: PMC8188158
- DOI: 10.1186/s12913-021-06509-x
Importance of patient bed pathways and length of stay differences in predicting COVID-19 hospital bed occupancy in England
Abstract
Background: Predicting bed occupancy for hospitalised patients with COVID-19 requires understanding of length of stay (LoS) in particular bed types. LoS can vary depending on the patient's "bed pathway" - the sequence of transfers of individual patients between bed types during a hospital stay. In this study, we characterise these pathways, and their impact on predicted hospital bed occupancy.
Methods: We obtained data from University College Hospital (UCH) and the ISARIC4C COVID-19 Clinical Information Network (CO-CIN) on hospitalised patients with COVID-19 who required care in general ward or critical care (CC) beds to determine possible bed pathways and LoS. We developed a discrete-time model to examine the implications of using either bed pathways or only average LoS by bed type to forecast bed occupancy. We compared model-predicted bed occupancy to publicly available bed occupancy data on COVID-19 in England between March and August 2020.
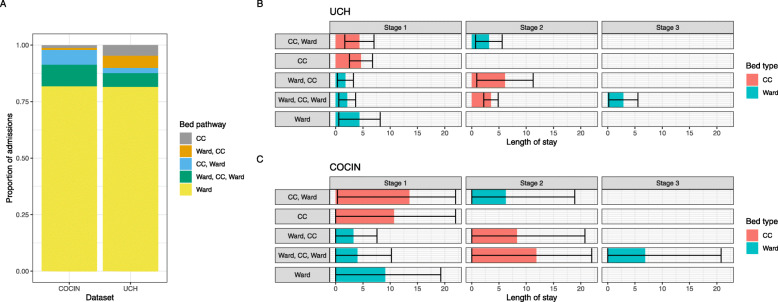
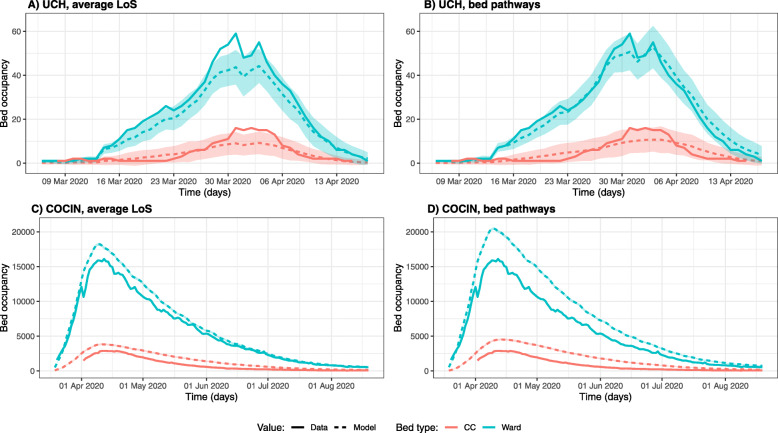
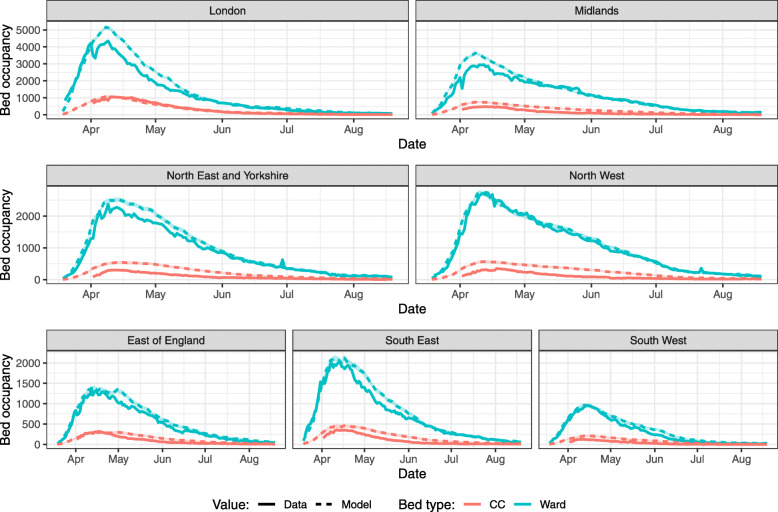
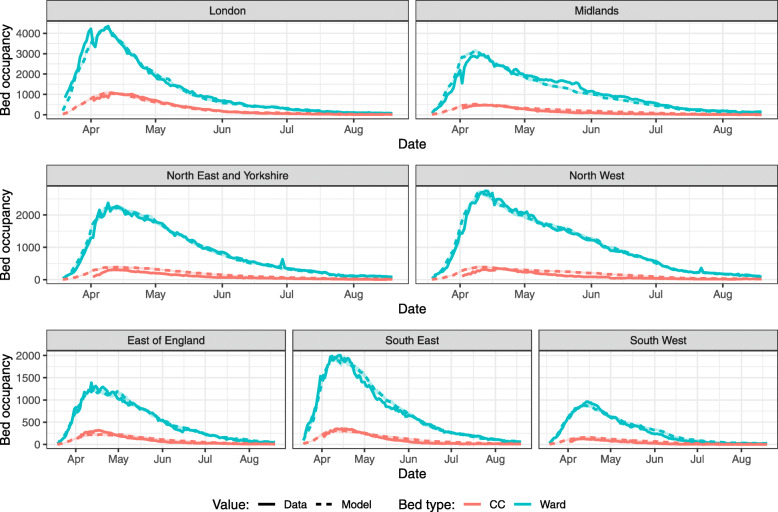
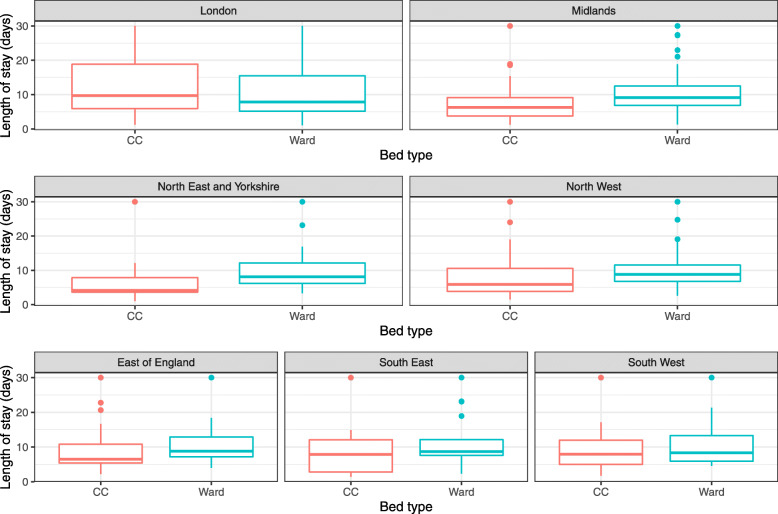
Results: In both the UCH and CO-CIN datasets, 82% of hospitalised patients with COVID-19 only received care in general ward beds. We identified four other bed pathways, present in both datasets: "Ward, CC, Ward", "Ward, CC", "CC" and "CC, Ward". Mean LoS varied by bed type, pathway, and dataset, between 1.78 and 13.53 days. For UCH, we found that using bed pathways improved the accuracy of bed occupancy predictions, while only using an average LoS for each bed type underestimated true bed occupancy. However, using the CO-CIN LoS dataset we were not able to replicate past data on bed occupancy in England, suggesting regional LoS heterogeneities.
Conclusions: We identified five bed pathways, with substantial variation in LoS by bed type, pathway, and geography. This might be caused by local differences in patient characteristics, clinical care strategies, or resource availability, and suggests that national LoS averages may not be appropriate for local forecasts of bed occupancy for COVID-19.
Trial registration: The ISARIC WHO CCP-UK study ISRCTN66726260 was retrospectively registered on 21/04/2020 and designated an Urgent Public Health Research Study by NIHR.
Keywords: Bed occupancy; Bed pathway; COVID-19; Hospitalisation; Length of stay; SARS-CoV-2.
Conflict of interest statement
MGS reports grants from DHSC NIHR UK, MRC UK, and HPRU in Emerging and Zoonotic Infections during the conduct of the study; minority ownership of Integrum Scientific LLC (Greensboro, NC, USA) outside the submitted work.
QJL, NMF, RHK, KDO, RS, KEA, SRP, GMK declare that they have no competing interests to disclose.
Figures
References
-
- Verity R, Okell LC, Dorigatti I, Winskill P, Whittaker C, Imai N, Cuomo-Dannenburg G, Thompson H, Walker PGT, Fu H, Dighe A, Griffin JT, Baguelin M, Bhatia S, Boonyasiri A, Cori A, Cucunubá Z, FitzJohn R, Gaythorpe K, Green W, Hamlet A, Hinsley W, Laydon D, Nedjati-Gilani G, Riley S, van Elsland S, Volz E, Wang H, Wang Y, Xi X, Donnelly CA, Ghani AC, Ferguson NM. Estimates of the severity of coronavirus disease 2019: a model-based analysis. Lancet Infect Dis. 2020;20(6):669–677. doi: 10.1016/S1473-3099(20)30243-7. - DOI - PMC - PubMed
-
- Statistics » Critical Care Bed Capacity and Urgent Operations Cancelled 2019-20 Data. [cited 2020 Sep 8]. Available from: https://www.england.nhs.uk/statistics/statistical-work-areas/critical-ca...
-
- Phua J, Weng L, Ling L, Egi M, Lim C-M, Divatia JV, Shrestha BR, Arabi YM, Ng J, Gomersall CD, Nishimura M, Koh Y, du B, Asian Critical Care Clinical Trials Group Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020;8(5):506–517. doi: 10.1016/S2213-2600(20)30161-2. - DOI - PMC - PubMed
MeSH terms
Grants and funding
- 206471/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- MR/S003975/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_19025/MRC_/Medical Research Council/United Kingdom
- 218554/Z/19//WT_/Wellcome Trust/United Kingdom
- MR/N013638/1/MRC_/Medical Research Council/United Kingdom
- G0701652/MRC_/Medical Research Council/United Kingdom
- BB/M009513/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- MR/P014658/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_19059/MRC_/Medical Research Council/United Kingdom
- MR/S032304/1/MRC_/Medical Research Council/United Kingdom
- MR/S017968/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
