

Sudden death in individuals with obstructive sleep apnoea: a systematic review and meta-analysis
- PMID: 34108135
- PMCID: PMC8191609
- DOI: 10.1136/bmjresp-2020-000656
Sudden death in individuals with obstructive sleep apnoea: a systematic review and meta-analysis
Abstract
Objectives: Over 1 billion individuals worldwide experience some form of sleep apnoea, and this number is steadily rising. Obstructive sleep apnoea (OSA) can negatively influence one's quality of life and potentially increase mortality risk. However, the association between OSA and mortality has not been reliably estimated. This meta-analysis estimates the risk of all-cause and cardiovascular mortality in individuals with OSA.
Design: Systematic review and meta-analysis.
Data sources: MEDLINE, Cochrane Library, Scopus and Joanna Briggs Institute Evidence-Based Practice databases were searched from inception through 1 January 2020.
Eligibility criteria for selecting studies: We included observational studies assessing the association of sudden deaths in individuals with and without OSA.
Data extraction and synthesis: Two independent reviewers (AES and ESH) extracted data and assessed the risk of bias using the Newcastle-Ottawa Scale quality assessment tool. Data were pooled using the random-effects models and reported as risk ratios (RRs) with 95% CIs. Heterogeneity was quantified with I2 statistic.
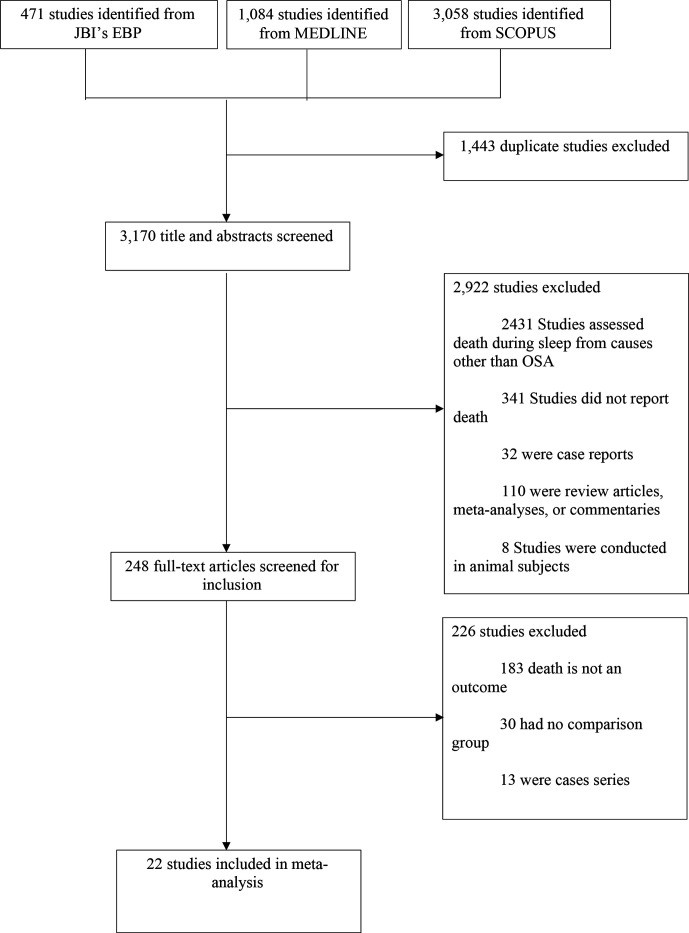
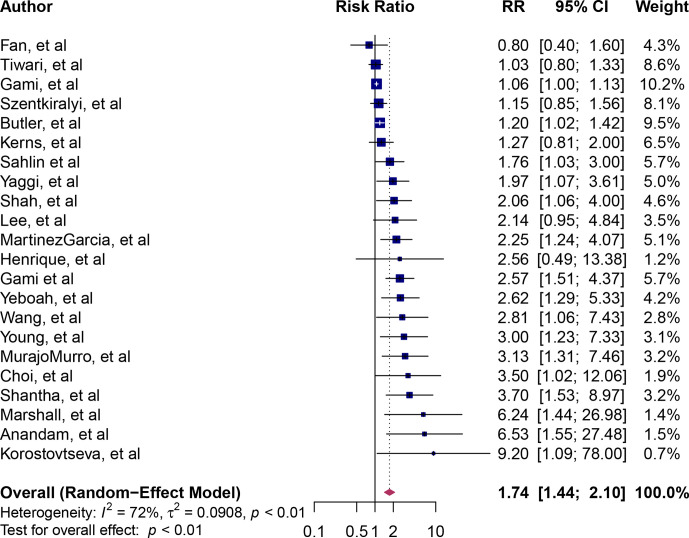
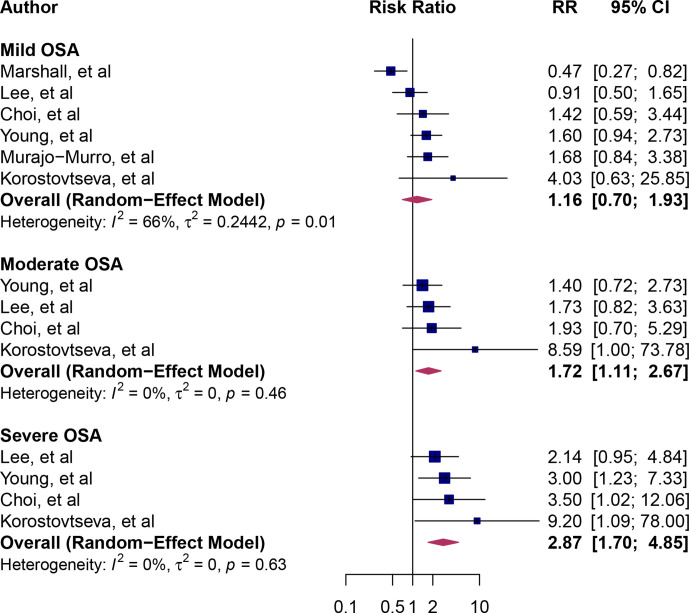
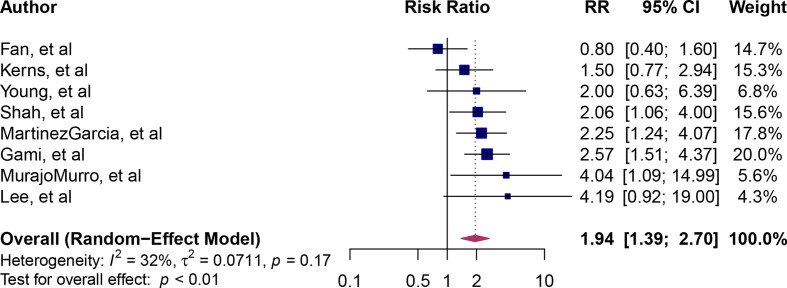
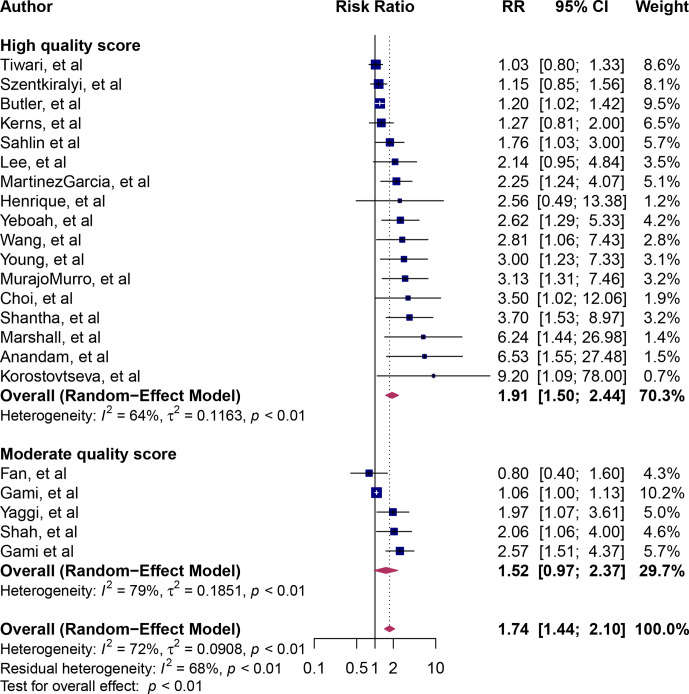
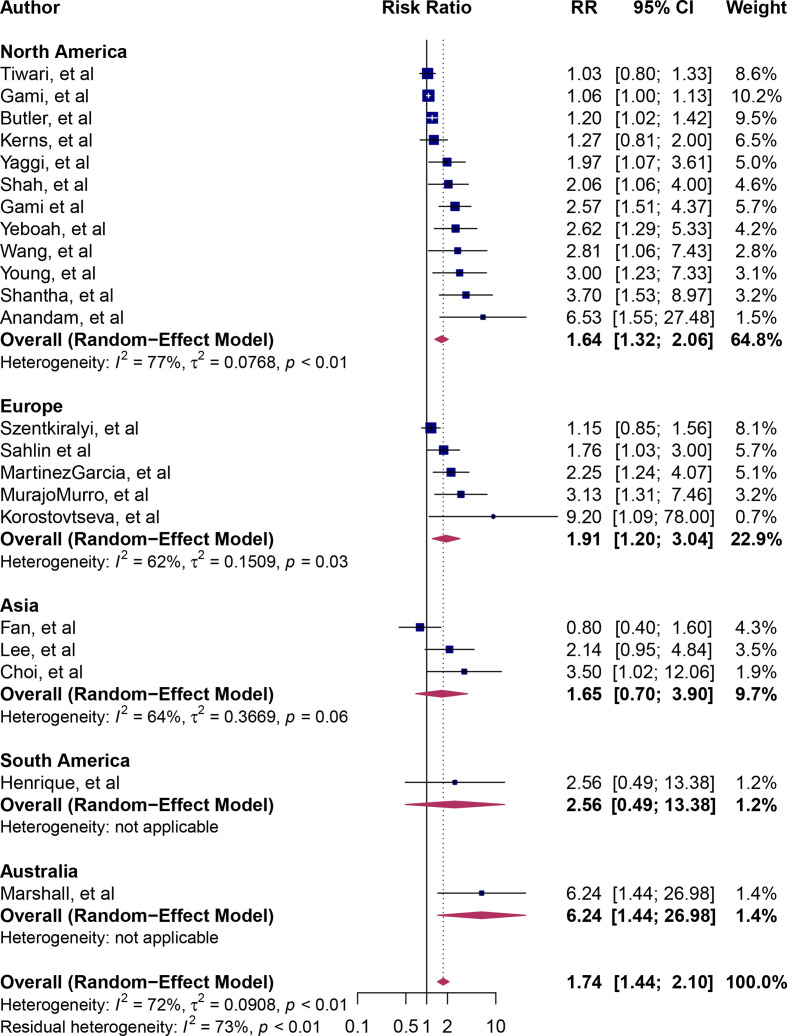
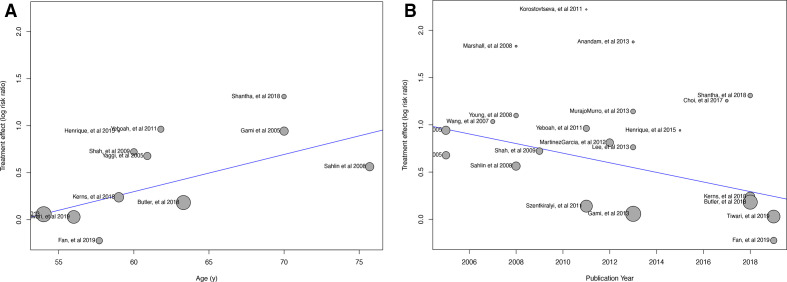
Results: We identified 22 observational studies (n=42 099 participants). The mean age was 62 years and 64% were men. OSA was associated with all-cause sudden death (RR=1.74, 95% CI: 1.44 to 2.10, I2=72%) and cardiovascular mortality (RR=1.94, 95% CI: 1.39 to 2.70, I2=32%). A marginally significant dose-response relationship between severity of OSA and the risk of death was observed (p for interaction=0.05): mild OSA (RR=1.16, 95% CI: 0.70 to 1.93), moderate OSA (RR=1.72, 95% CI: 1.11 to 2.67) and severe OSA (RR=2.87, 95% CI: 1.70 to 4.85). Meta-regression analysis showed that older age was a significant contributing factor in the relationship between OSA and mortality. The median study methodological quality was considered high.
Conclusions: OSA is a significant risk factor for all-cause mortality and cardiac mortality. Prevention and treatment strategies to optimise survival and quality of life in individuals with OSA are urgently needed.
Prospero registration number: CRD42020164941.
Keywords: clinical epidemiology; sleep apnoea.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical