

Variable immunodeficiency score upfront analytical link (VISUAL), a proposal for combined prognostic score at diagnosis of common variable immunodeficiency
- PMID: 34108596
- PMCID: PMC8190250
- DOI: 10.1038/s41598-021-91791-2
Variable immunodeficiency score upfront analytical link (VISUAL), a proposal for combined prognostic score at diagnosis of common variable immunodeficiency
Abstract
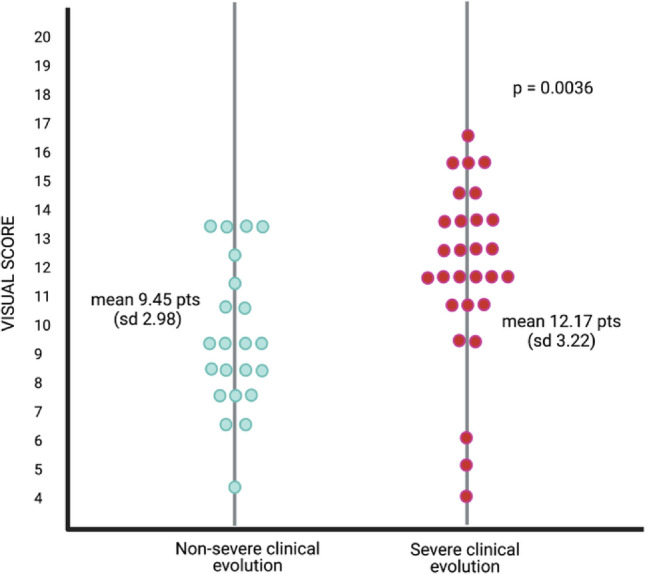
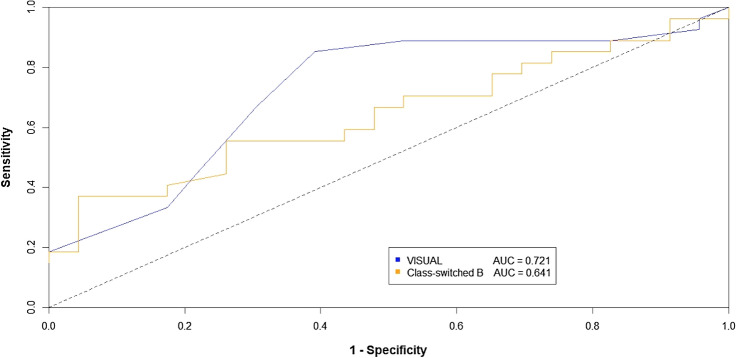
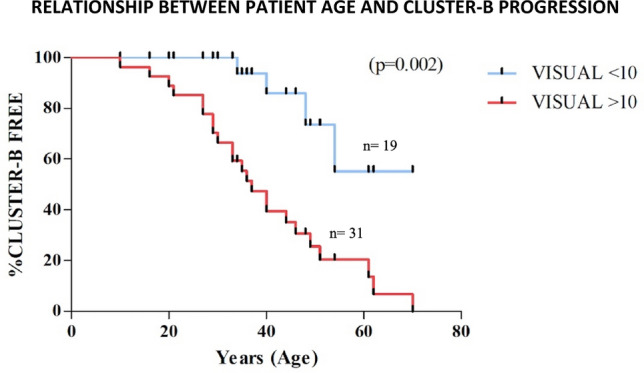
The broad and heterogeneous clinical spectrum that characterizes common variable immunodeficiency (CVID) is associated with quite different disease course and prognosis, highlighting the need to develop tools that predict complications. We developed a multianalyte VISUAL score (variable immunodeficiency score upfront analytical link) aimed to predict severity using individual CVID patient data at baseline of a cohort of 50 CVID patients from two different centers in Portugal and Spain. We retrospectively applied VISUAL to the CVID clinical severity scores proposed by Ameratunga and Grimbacher after 15 years follow-up of our cohort. VISUAL score at CVID diagnosis showed adequate performance for predicting infectious and non-infectious severe complications (Cluster B). Compared to switched memory B lymphocyte phenotype alone, VISUAL provided a more accurate identification of clinically meaningful outcome, with significantly higher sensitivity (85% vs 55%, p = 0.01), and negative predictive value (77% vs 58%) and AUC of the ROC curves (0.72 vs 0.64), with optimal cut-off level of 10. For every increase of 1 point in the VISUAL scale, the odds of being in the higher risk category (Cluster B) increased in 1.3 (p = 0.005) for Ameratunga's severity score and 1.26 (p = 0.004) for Grimbacher's severity score. At diagnosis of CVID, VISUAL score ≥ 10 showed 8.94-fold higher odds of severe prognosis than below this threshold. Kaplan-Meier estimates for the VISUAL ≥ 10 points showed significantly earlier progression to Cluster B than those with VISUAL < 10 (p = 0.0002). This prognostic laboratory score might allow close monitoring and more aggressive treatment in patients with scores ≥ 10 on a personalized basis approach. Further studies are needed to prospectively validate VISUAL score.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Siachoque H, Satisteban N, Iglesias-Gamarra A. T regulatory lymphocytes: Subpopulations, mechanism of action and importance in the control of autoimmunity. Rev. Colomb. Reumatol. 2011;18:203–220.
MeSH terms
LinkOut - more resources
Full Text Sources
