

The Effect of Congenital and Acquired Bilateral Anophthalmia on Brain Structure
- PMID: 34108778
- PMCID: PMC8158038
- DOI: 10.1080/01658107.2020.1856143
The Effect of Congenital and Acquired Bilateral Anophthalmia on Brain Structure
Abstract
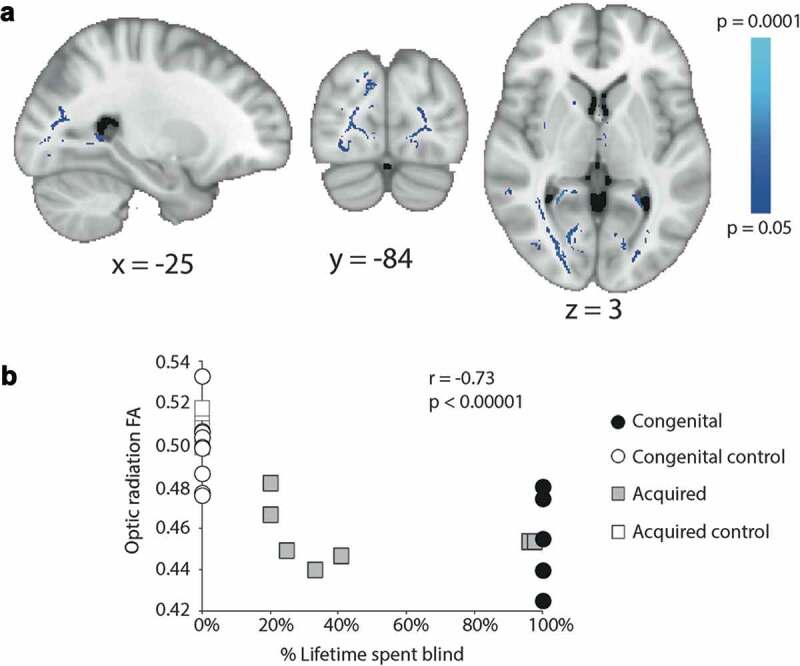
The aim of this study was to compare the pattern of changes in brain structure resulting from congenital and acquired bilateral anophthalmia. Brain structure was investigated using 3T magnetic resonance imaging (MRI) in Oxford (congenital) or Manchester (acquired). T1-weighted structural and diffusion-weighted scans were acquired from people with anophthalmia and sighted control participants. Differences in grey matter between the groups were quantified using voxel-based morphometry and differences in white matter microstructure using tract-based spatial statistics. Quantification of optic nerve volume and cortical thickness in visual regions was also performed in all groups. The optic nerve was reduced in volume in both anophthalmic populations, but to a greater extent in the congenital group and anophthalmia acquired at an early age. A similar pattern was found for the white matter microstructure throughout the occipitotemporal regions of the brain, suggesting a greater reduction of integrity with increasing duration of anophthalmia. In contrast, grey matter volume changes differed between the two groups, with the acquired anophthalmia group showing a decrease in the calcarine sulcus, corresponding to the area that would have been peripheral primary visual cortex. In contrast, the acquired anophthalmia group showed a decrease in grey matter volume in the calcarine sulcus corresponding to the area that would have been peripheral primary visual cortex. There are both qualitative and quantitative differences in structural brain changes in congenital and acquired anophthalmia, indicating differential effects of development and degeneration.
Keywords: Anophthalmia; cortical thickness; diffusion imaging; grey matter; magnetic resonance imaging; optic nerve.
© 2021 The Author(s). Published with license by Taylor & Francis Group, LLC.
Figures




References
Grants and funding
LinkOut - more resources
Full Text Sources