

Replication and cross-validation of type 2 diabetes subtypes based on clinical variables: an IMI-RHAPSODY study
- PMID: 34110439
- PMCID: PMC8382625
- DOI: 10.1007/s00125-021-05490-8
Replication and cross-validation of type 2 diabetes subtypes based on clinical variables: an IMI-RHAPSODY study
Abstract
Aims/hypothesis: Five clusters based on clinical characteristics have been suggested as diabetes subtypes: one autoimmune and four subtypes of type 2 diabetes. In the current study we replicate and cross-validate these type 2 diabetes clusters in three large cohorts using variables readily measured in the clinic.
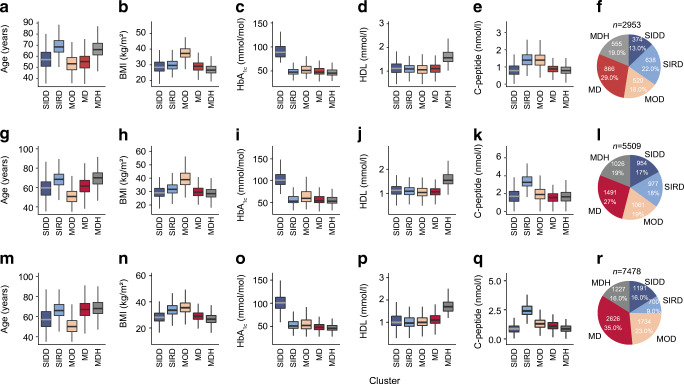
Methods: In three independent cohorts, in total 15,940 individuals were clustered based on age, BMI, HbA1c, random or fasting C-peptide, and HDL-cholesterol. Clusters were cross-validated against the original clusters based on HOMA measures. In addition, between cohorts, clusters were cross-validated by re-assigning people based on each cohort's cluster centres. Finally, we compared the time to insulin requirement for each cluster.
Results: Five distinct type 2 diabetes clusters were identified and mapped back to the original four All New Diabetics in Scania (ANDIS) clusters. Using C-peptide and HDL-cholesterol instead of HOMA2-B and HOMA2-IR, three of the clusters mapped with high sensitivity (80.6-90.7%) to the previously identified severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD) and mild obesity-related diabetes (MOD) clusters. The previously described ANDIS mild age-related diabetes (MARD) cluster could be mapped to the two milder groups in our study: one characterised by high HDL-cholesterol (mild diabetes with high HDL-cholesterol [MDH] cluster), and the other not having any extreme characteristic (mild diabetes [MD]). When these two milder groups were combined, they mapped well to the previously labelled MARD cluster (sensitivity 79.1%). In the cross-validation between cohorts, particularly the SIDD and MDH clusters cross-validated well, with sensitivities ranging from 73.3% to 97.1%. SIRD and MD showed a lower sensitivity, ranging from 36.1% to 92.3%, where individuals shifted from SIRD to MD and vice versa. People belonging to the SIDD cluster showed the fastest progression towards insulin requirement, while the MDH cluster showed the slowest progression.
Conclusions/interpretation: Clusters based on C-peptide instead of HOMA2 measures resemble those based on HOMA2 measures, especially for SIDD, SIRD and MOD. By adding HDL-cholesterol, the MARD cluster based upon HOMA2 measures resulted in the current clustering into two clusters, with one cluster having high HDL levels. Cross-validation between cohorts showed generally a good resemblance between cohorts. Together, our results show that the clustering based on clinical variables readily measured in the clinic (age, HbA1c, HDL-cholesterol, BMI and C-peptide) results in informative clusters that are representative of the original ANDIS clusters and stable across cohorts. Adding HDL-cholesterol to the clustering resulted in the identification of a cluster with very slow glycaemic deterioration.
Keywords: C-peptide; Clusters; Cross-validation; HDL-cholesterol; Type 2 diabetes.
© 2021. The Author(s).
Figures
References
-
- Safai N, Ali A, Rossing P, Ridderstråle M (2018) Stratification of type 2 diabetes based on routine clinical markers. Diabetes Res Clin Pract 141:275–283. 10.1016/j.diabres.2018.05.014 - PubMed
-
- Dennis JM, Shields BM, Henley WE, Jones AG, Hattersley AT. Disease progression and treatment response in data-driven subgroups of type 2 diabetes compared with models based on simple clinical features: an analysis using clinical trial data. Lancet Diabetes Endocrinol. 2019;7(6):442–451. doi: 10.1016/S2213-8587(19)30087-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
