

Tobacco use in the Myeloproliferative neoplasms: symptom burden, patient opinions, and care
- PMID: 34112113
- PMCID: PMC8194237
- DOI: 10.1186/s12885-021-08439-7
Tobacco use in the Myeloproliferative neoplasms: symptom burden, patient opinions, and care
Abstract
Background: Patients with Philadelphia-negative Myeloproliferative Neoplasms (MPN) suffer from numerous symptoms and decreased quality of life. Smoking is associated with an increased symptom burden in several malignancies. The aim of this study was to analyze the association between smoking and MPN-related symptom burden and explore MPN patients' opinions on smoking.
Methods: A total of 435 patients with MPN participated in a cross-sectional internet-based survey developed by the Mayo Clinic and the Myeloproliferative Neoplasm Quality of Life Group. Patients reported their demographics, disease characteristics, tobacco use, and opinions on tobacco use. In addition, MPN-related symptoms were reported via the validated 10-item version of the Myeloproliferative Neoplasms Symptom Assessment Form.
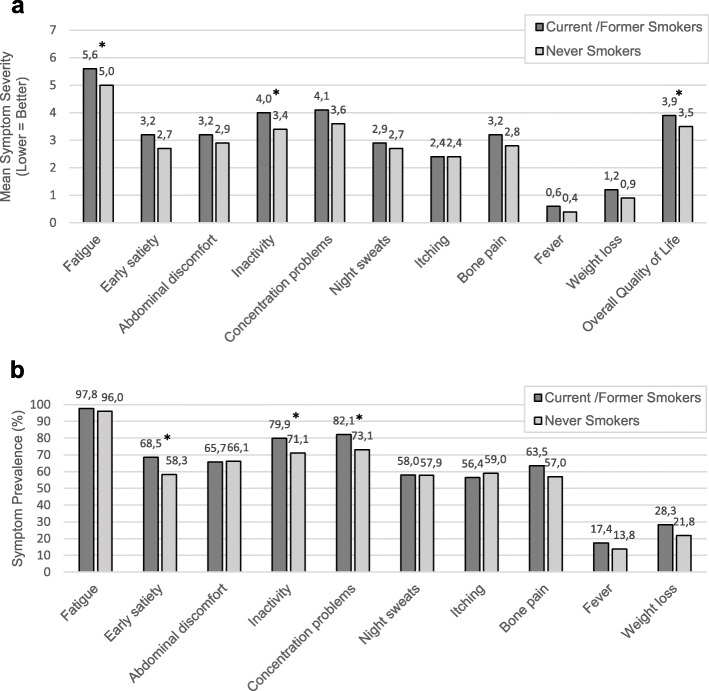
Results: Current/former smokers reported worse fatigue (mean severity 5.6 vs. 5.0, p = 0.02) and inactivity (mean severity 4.0 vs. 3.4, p = 0.03) than never smokers. Moreover, current/former smokers more frequently experienced early satiety (68.5% vs. 58.3%, p = 0.03), inactivity (79.9% vs. 71.1%, p = 0.04), and concentration difficulties (82.1% vs. 73.1%, p = 0.04). Although not significant, a higher total symptom burden was observed for current/former smokers (mean 30.4 vs. 27.0, p = 0.07). Accordingly, overall quality of life was significantly better among never smokers than current/former smokers (mean 3.5 vs. 3.9, p = 0.03). Only 43.2% of the current/former smokers reported having discussed tobacco use with their physician, and 17.5% did not believe smoking increased the risk of thrombosis.
Conclusion: The current study suggests that smoking may be associated with increased prevalence and severity of MPN symptoms and underscores the need to enhance patient education and address tobacco use in the care of MPN patients.
Keywords: Cross-sectional internet-based survey; Myeloproliferative neoplasms; Quality of life; Symptom burden; Tobacco use.
Conflict of interest statement
Ruben Mesa: Consultant - Novartis, Sierra, La Jolla, Pharma; Research Support – Incyte, CTI, Celgene, Abbvie, Samus, Promedior, Genetech; Robyn Scherber: Employment – Incyte; Hans Hasselbalch: Consultant – Novartis; Advisory Board – AOP Orphan; Research Grant – Novartis.
Figures

References
-
- U.S. Department of Health and Human Services, The Health Consequences of Smoking- 50 Years of Progress: A Report of the Surgeon General, 2014. http://www.cdc.gov/tobacco/data_statistics/sgr/50th-anniversary/index.htm. Accessed 2 May 2019.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
