

Demographic, multi-morbidity and genetic impact on myocardial involvement and its recovery from COVID-19: protocol design of COVID-HEART-a UK, multicentre, observational study
- PMID: 34112195
- PMCID: PMC8190746
- DOI: 10.1186/s12968-021-00752-1
Demographic, multi-morbidity and genetic impact on myocardial involvement and its recovery from COVID-19: protocol design of COVID-HEART-a UK, multicentre, observational study
Abstract
Background: Although coronavirus disease 2019 (COVID-19) is primarily a respiratory illness, myocardial injury is increasingly reported and associated with adverse outcomes. However, the pathophysiology, extent of myocardial injury and clinical significance remains unclear.
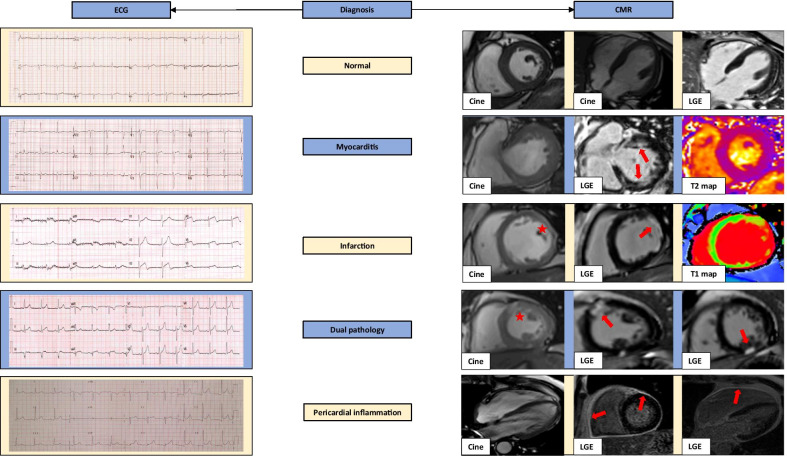
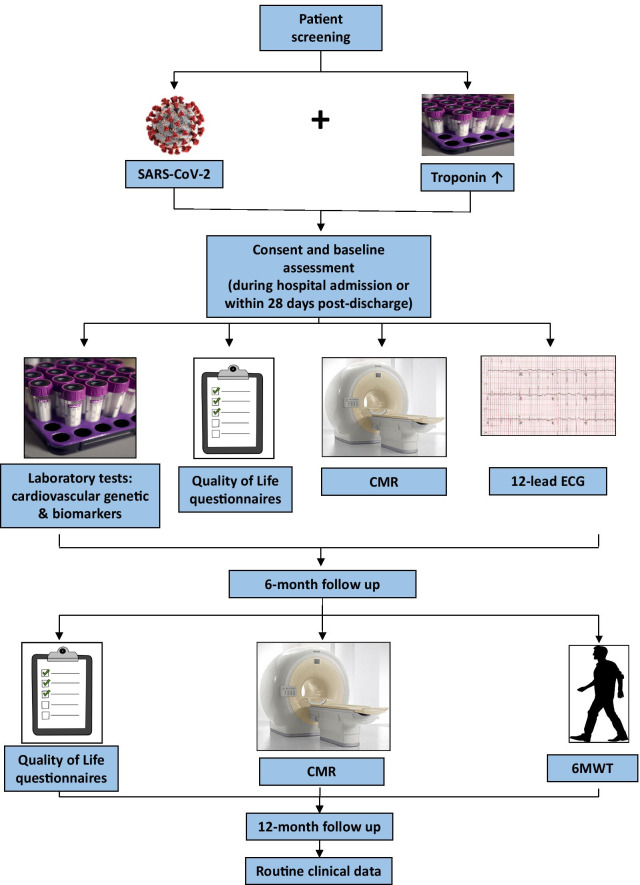
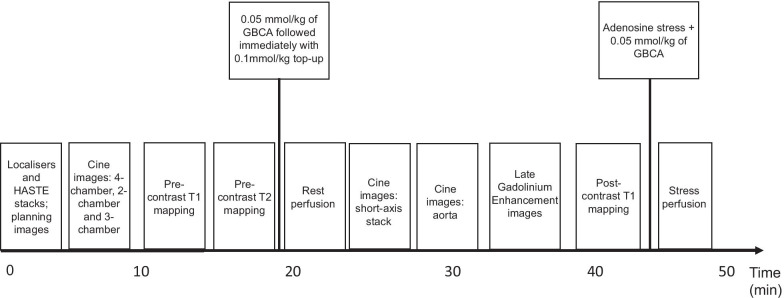
Methods: COVID-HEART is a UK, multicentre, prospective, observational, longitudinal cohort study of patients with confirmed COVID-19 and elevated troponin (sex-specific > 99th centile). Baseline assessment will be whilst recovering in-hospital or recently discharged, and include cardiovascular magnetic resonance (CMR) imaging, quality of life (QoL) assessments, electrocardiogram (ECG), serum biomarkers and genetics. Assessment at 6-months includes repeat CMR, QoL assessments and 6-min walk test (6MWT). The CMR protocol includes cine imaging, T1/T2 mapping, aortic distensibility, late gadolinium enhancement (LGE), and adenosine stress myocardial perfusion imaging in selected patients. The main objectives of the study are to: (1) characterise the extent and nature of myocardial involvement in COVID-19 patients with an elevated troponin, (2) assess how cardiac involvement and clinical outcome associate with recognised risk factors for mortality (age, sex, ethnicity and comorbidities) and genetic factors, (3) evaluate if differences in myocardial recovery at 6 months are dependent on demographics, genetics and comorbidities, (4) understand the impact of recovery status at 6 months on patient-reported QoL and functional capacity.
Discussion: COVID-HEART will provide detailed characterisation of cardiac involvement, and its repair and recovery in relation to comorbidity, genetics, patient-reported QoL measures and functional capacity.
Clinical trial registration: ISRCTN 58667920. Registered 04 August 2020.
Keywords: COVID-19; Cardiovascular disease; Cardiovascular magnetic resonance; Coronavirus; Myocardial infarction; Myocardial inflammation; Myocardial repair; Myocarditis; Myopericarditis; myocardial injury.
Conflict of interest statement
CB is employed by the University of Glasgow which holds research and/or consultancy agreements with AstraZeneca, Abbott Vascular, Boehringer Ingelheim, GSK, HeartFlow, Opsens, and Novartis. CBD is the chief executive officer (part-time) of the Society for Cardiovascular Magnetic Resonance (SCMR). All other authors have no conflicts to declare.
Figures
References
-
- Raman B, Cassar MP, Tunnicliffe EM, Filippini N, Griffanti L, Alfaro-Almagro F, et al. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine. 2020;31:100683. doi: 10.1016/j.eclinm.2020.100683. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
