

The ARIC (Atherosclerosis Risk In Communities) Study: JACC Focus Seminar 3/8
- PMID: 34112321
- PMCID: PMC8667593
- DOI: 10.1016/j.jacc.2021.04.035
The ARIC (Atherosclerosis Risk In Communities) Study: JACC Focus Seminar 3/8
Abstract
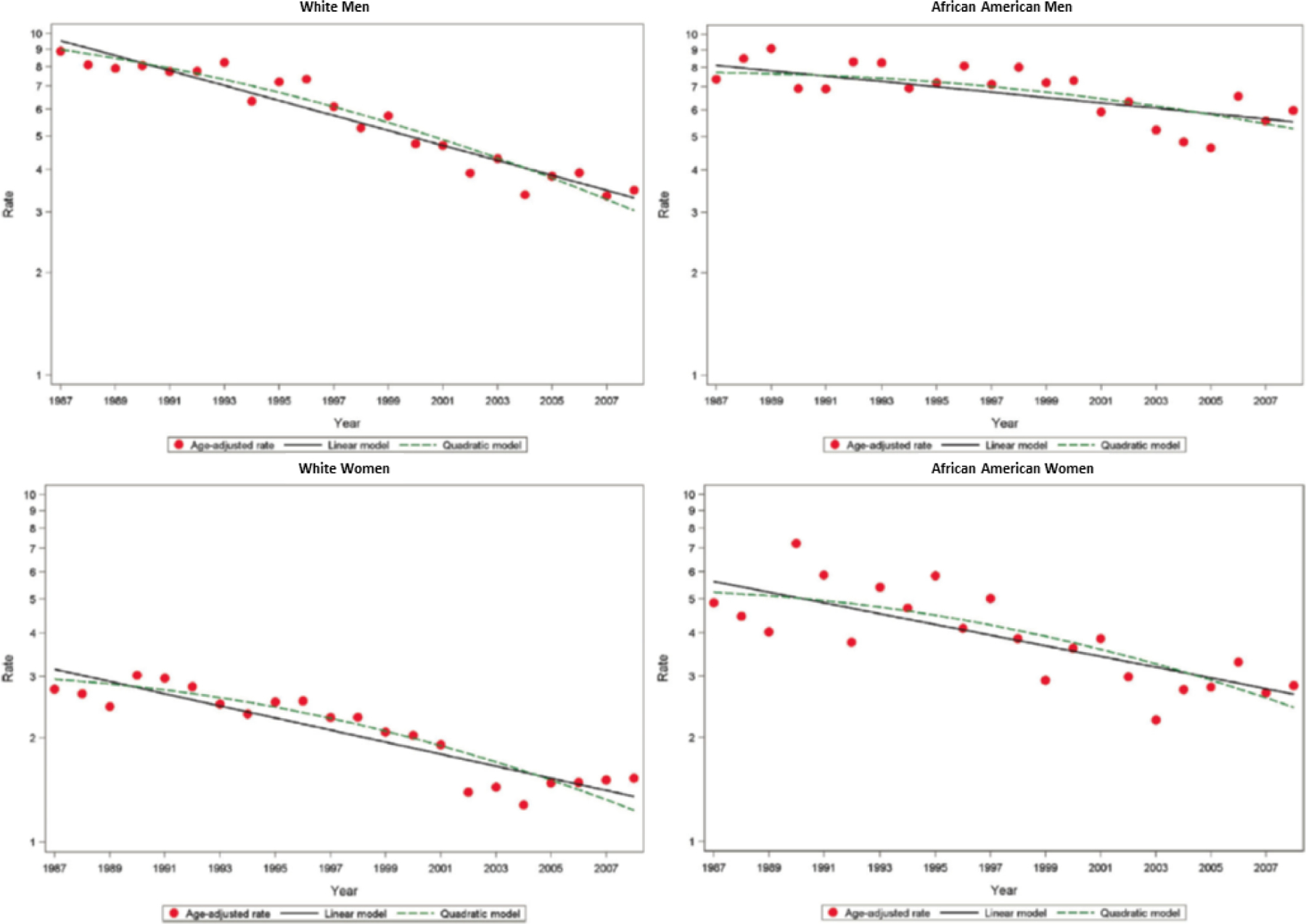
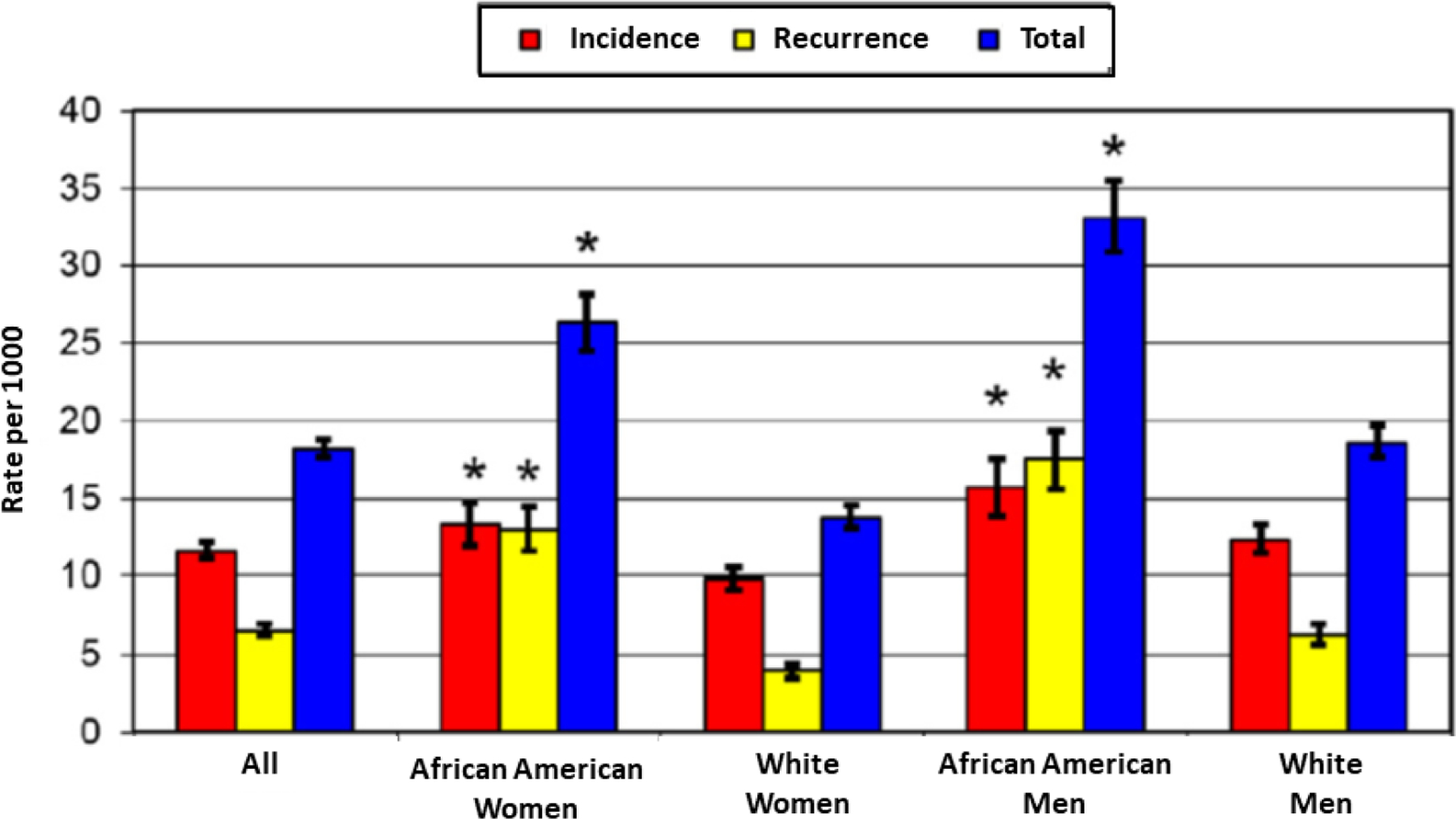
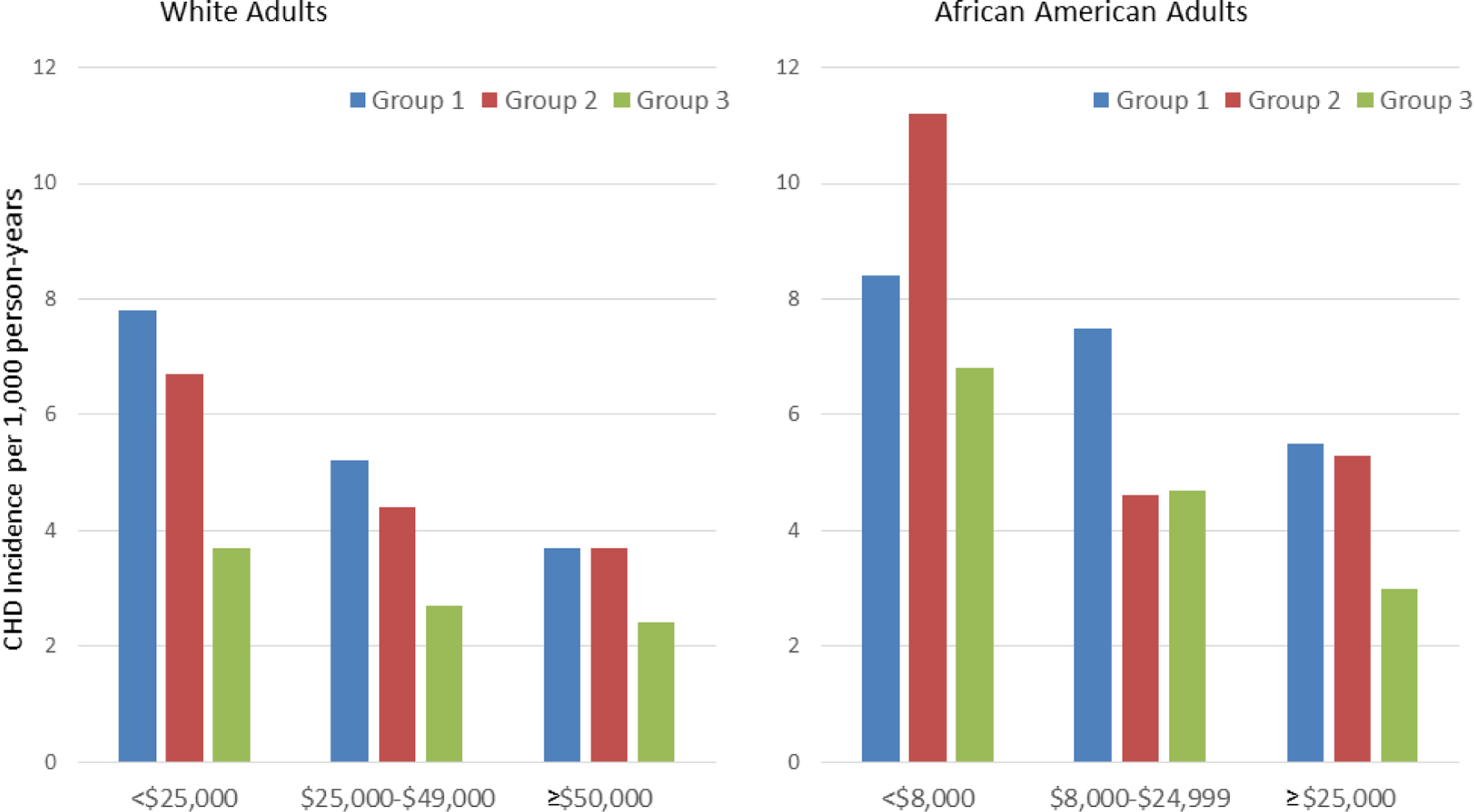
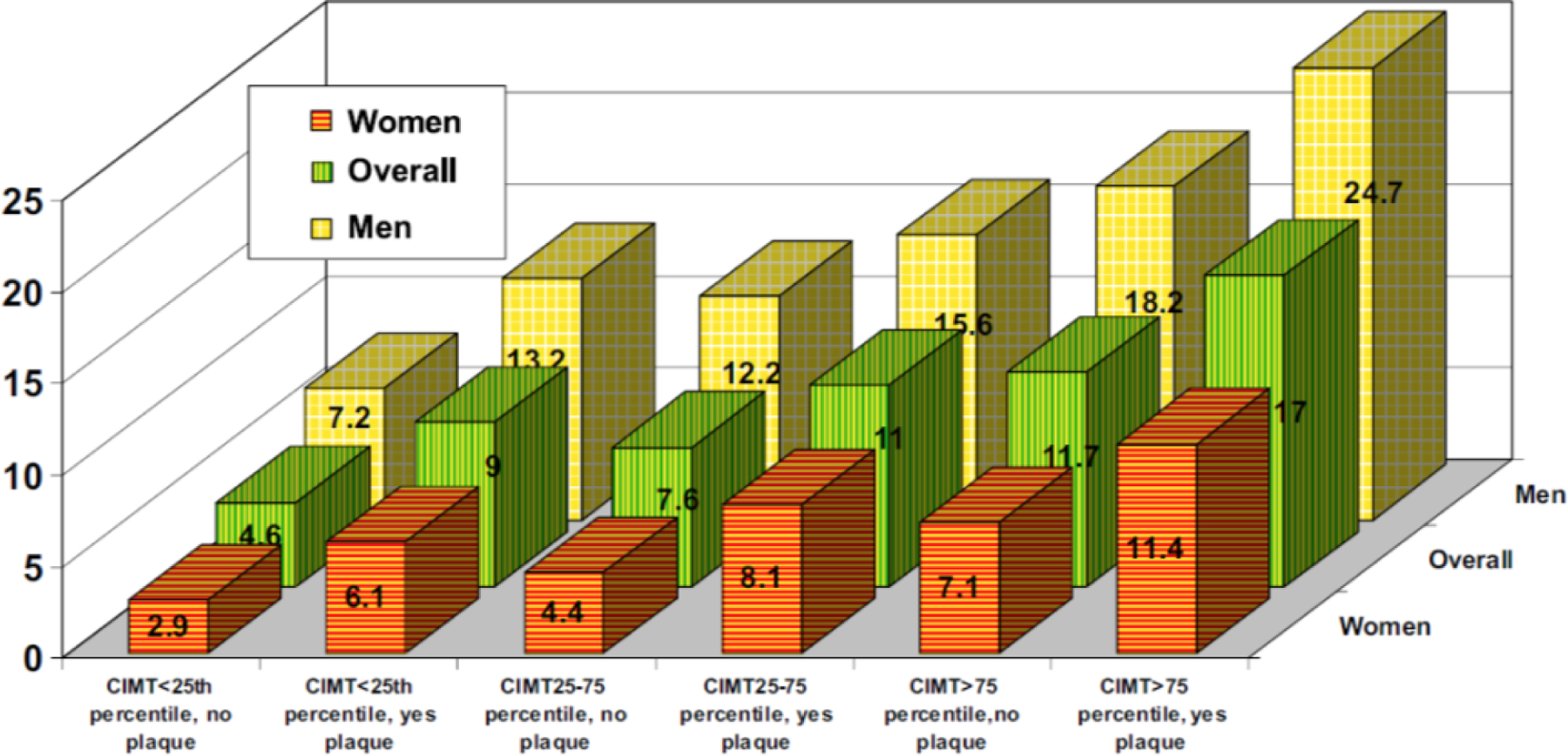
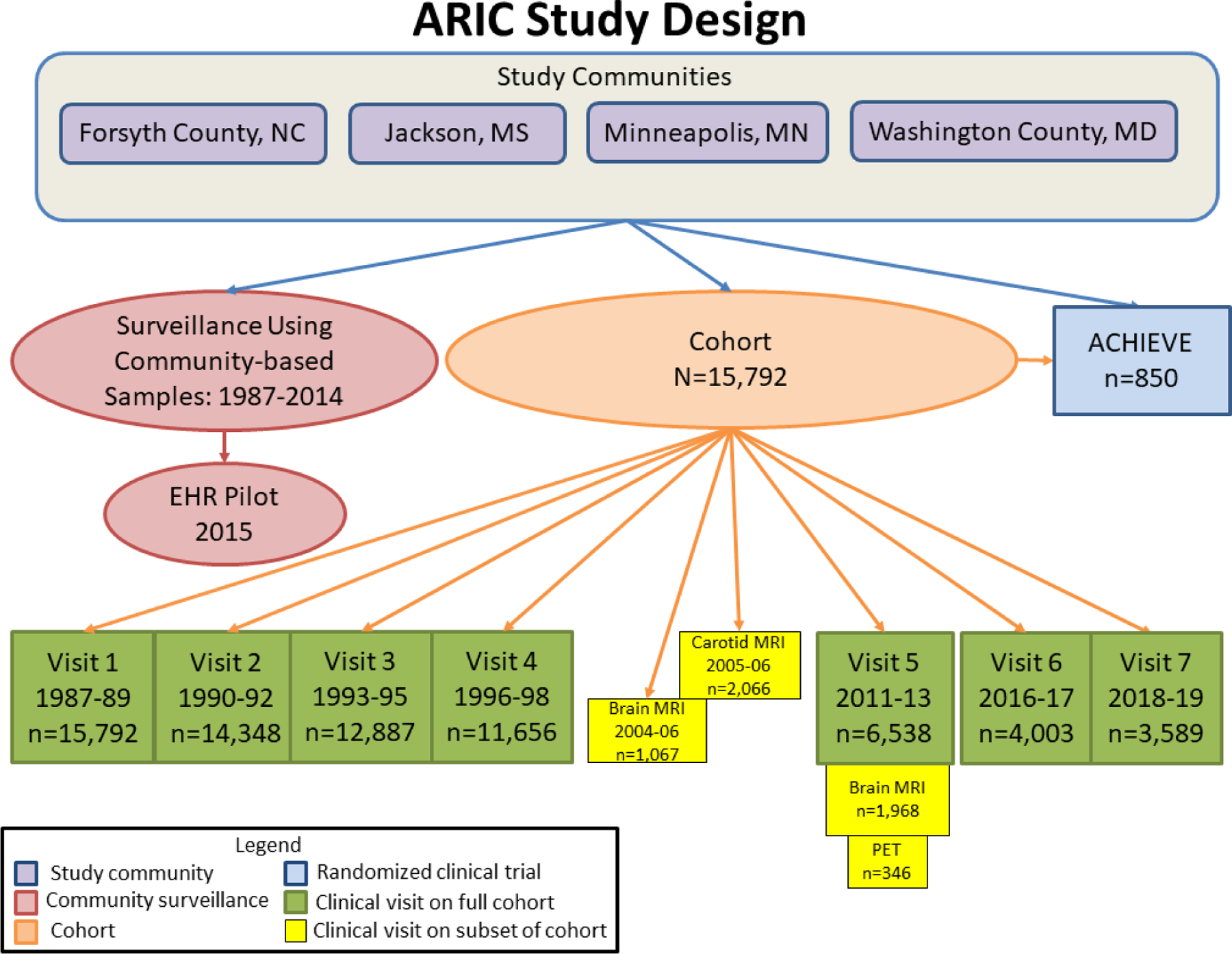
ARIC (Atherosclerosis Risk In Communities) initiated community-based surveillance in 1987 for myocardial infarction and coronary heart disease (CHD) incidence and mortality and created a prospective cohort of 15,792 Black and White adults ages 45 to 64 years. The primary aims were to improve understanding of the decline in CHD mortality and identify determinants of subclinical atherosclerosis and CHD in Black and White middle-age adults. ARIC has examined areas including health disparities, genomics, heart failure, and prevention, producing more than 2,300 publications. Results have had strong clinical impact and demonstrate the importance of population-based research in the spectrum of biomedical research to improve health.
Keywords: adult; cohort study; epidemiology; health disparity; risk factors; surveillance.
Published by Elsevier Inc.
Conflict of interest statement
Funding Support and Author Disclosures The ARIC study has been funded in whole or in part with federal funds from the National Heart, Lung, and Blood Institute, National Institutes of Health, Department of Health and Human Services, under contract nos. HHSN268201700001I, HHSN268201700002I, HHSN268201700003I, HHSN268201700004I, and HHSN268201700005I. Neurocognitive data are collected by U01 2U01HL096812, 2U01HL096814, 2U01HL096899, 2U01HL096902, and 2U01HL096917 from the National Institutes of Health (National Heart, Lung, and Blood Institute; National Institute of Neurological Disorders and Stroke; National Institute on Aging; and National Institute on Deafness and Other Communication Disorders) and with previous brain magnetic resonance imaging examinations funded by R01-HL70825 and biomarkers by R01-HL134320 from the National Heart, Lung, and Blood Institute. Dr. Coresh has received investigator-initiated grant support from the National Institutes of Health and National Kidney Foundation (the National Kidney Foundation received research support from industry) and has served as a scientific advisor to Healthy.io and Alike. Dr. Ballantyne has received significant (>$10,000) grant/research support (all paid to institution, not individual) from Abbott Diagnostic, Akcea, Amgen, Esperion, Novartis, Regeneron, Roche Diagnostic, the National Institutes of Health, the American Heart Association, and American Diabetes Association; and has served as a consultant for Abbott Diagnostics, Akcea, Althera, Amarin (significant), Amgen, Arrowhead, AstraZeneca, Corvidia, Denka Seiken (significant), Esperion, Gilead, Janssen, Matinas BioPharma Inc., New Amsterdam (significant), Novartis, Novo Nordisk, Pfizer, Regeneron, Roche Diagnostic, and Sanofi-Synthelabo (significant). All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- The ARIC Investigators. The Atherosclerosis Risk in Communities (ARIC) study: design and objectives. Am J Epidemiol 1989;129:687–702. - PubMed
-
- Havlik RJ, Feinleib M, editors. Proceedings of the 1978 Conference on the Decline in Coronary Heart Disease Mortality. Bethesda, MD: U.S. Department of Health, Education, and Welfare, Public Health Service, National Institutes of Health, 1979.
-
- CCSP Coordinating Center. Community Cardiovascular Surveillance Program: Final Report to the National Heart, Lung, and Blood Institute. University of Maryland; Baltimore MD: 1984.
Publication types
MeSH terms
Grants and funding
- U01 HL096812/HL/NHLBI NIH HHS/United States
- R01 HL131136/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
- R01 HL134320/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
