

Analysis of multispectral imaging with the AstroPath platform informs efficacy of PD-1 blockade
- PMID: 34112666
- PMCID: PMC8709533
- DOI: 10.1126/science.aba2609
Analysis of multispectral imaging with the AstroPath platform informs efficacy of PD-1 blockade
Abstract
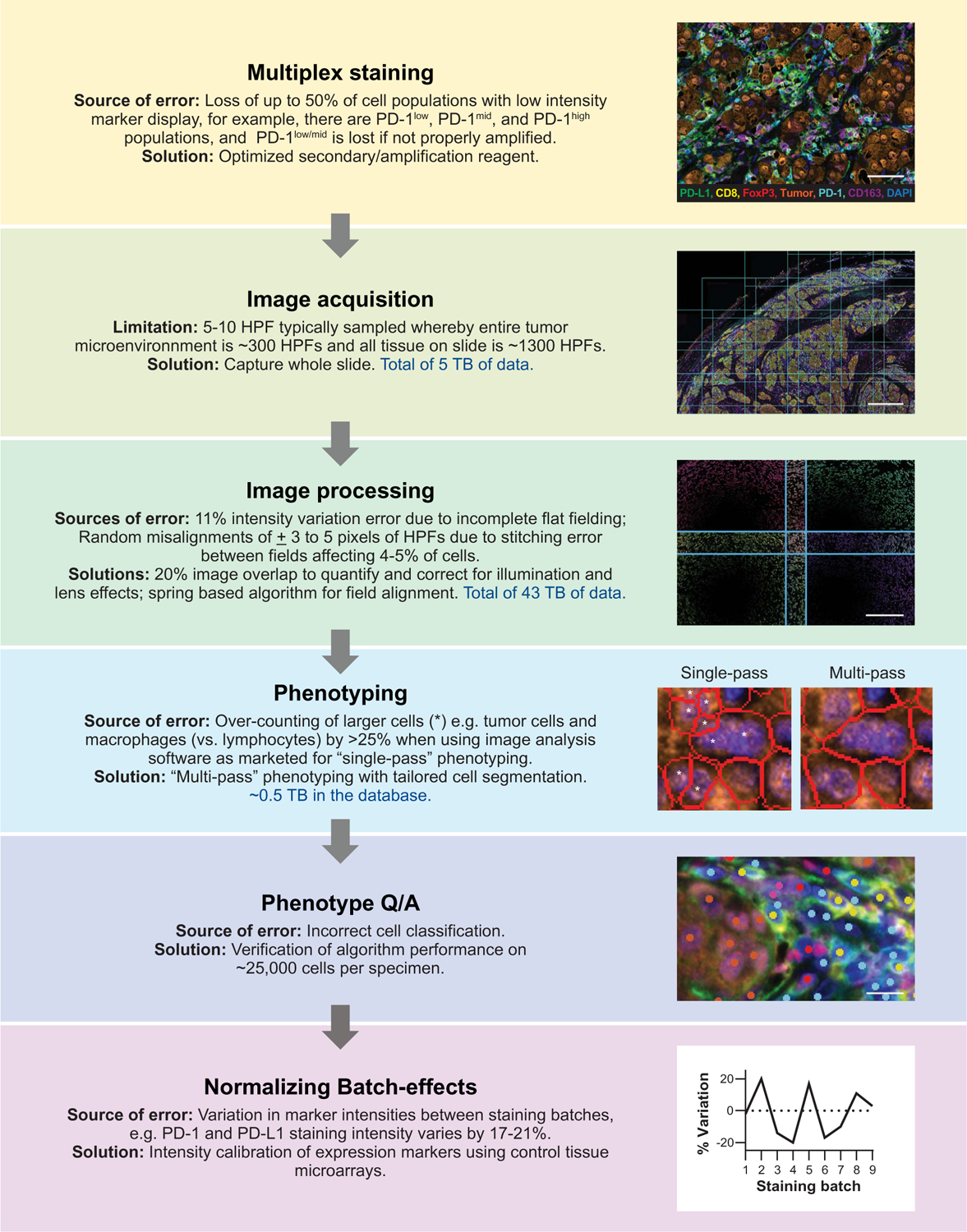
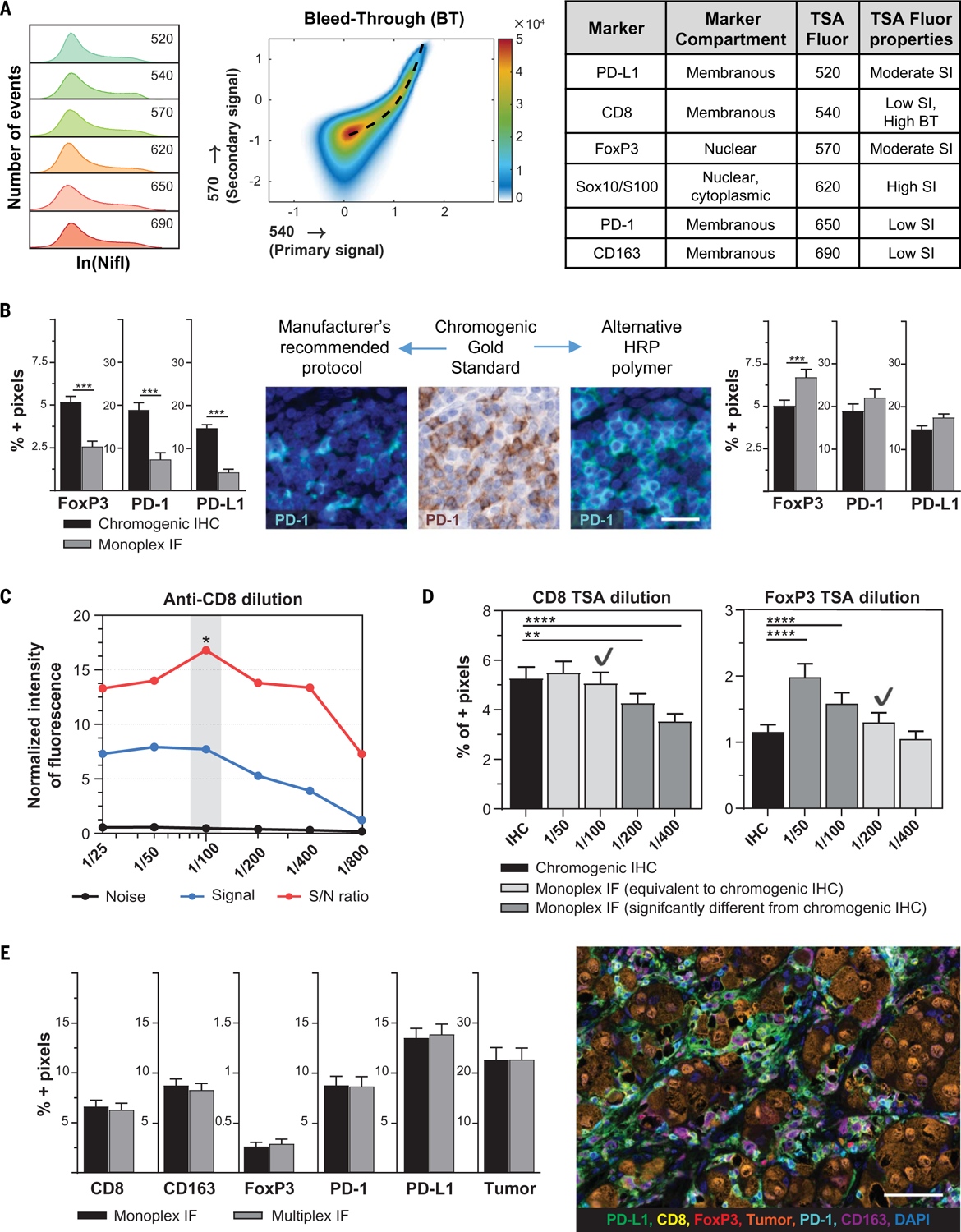
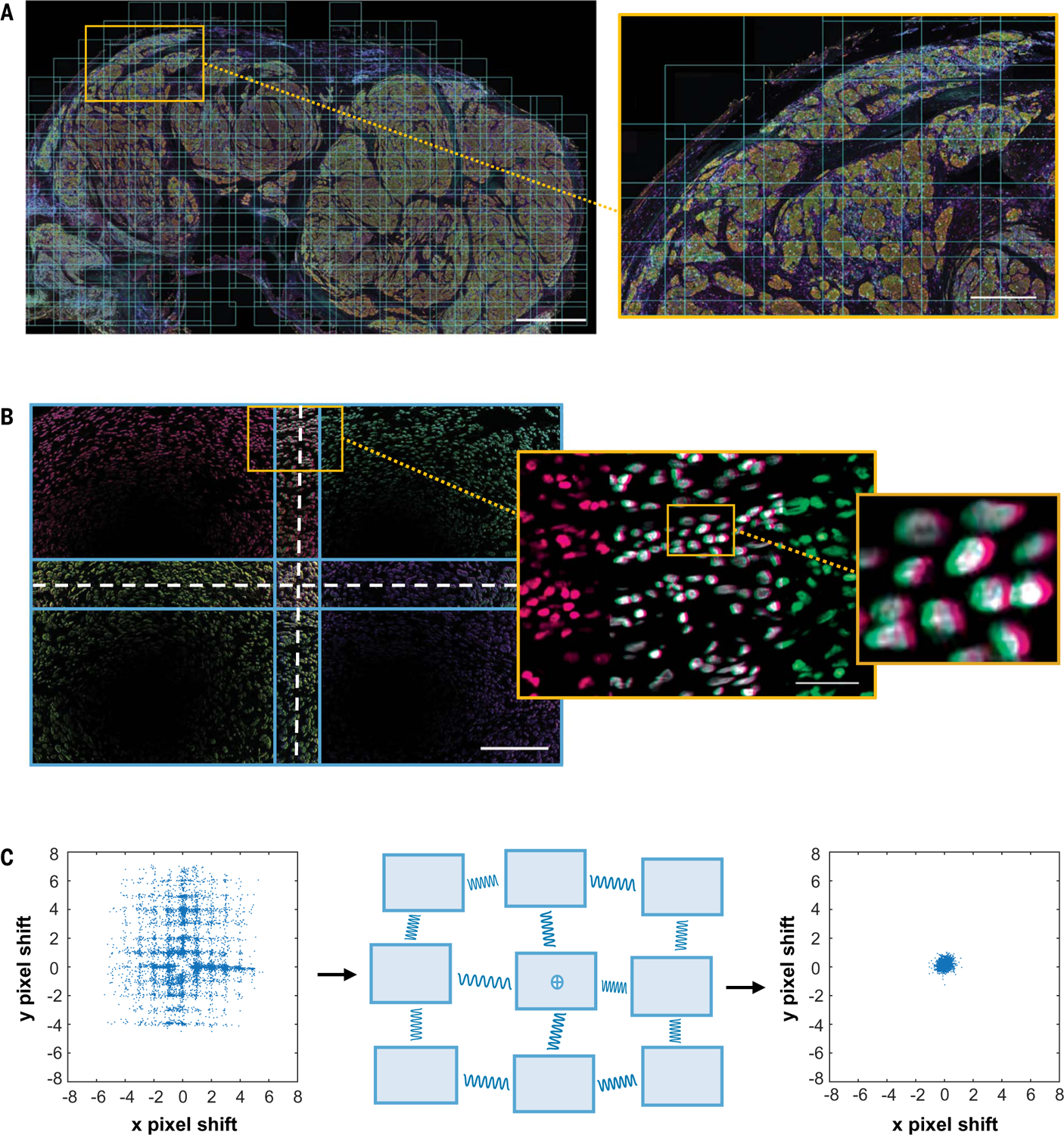
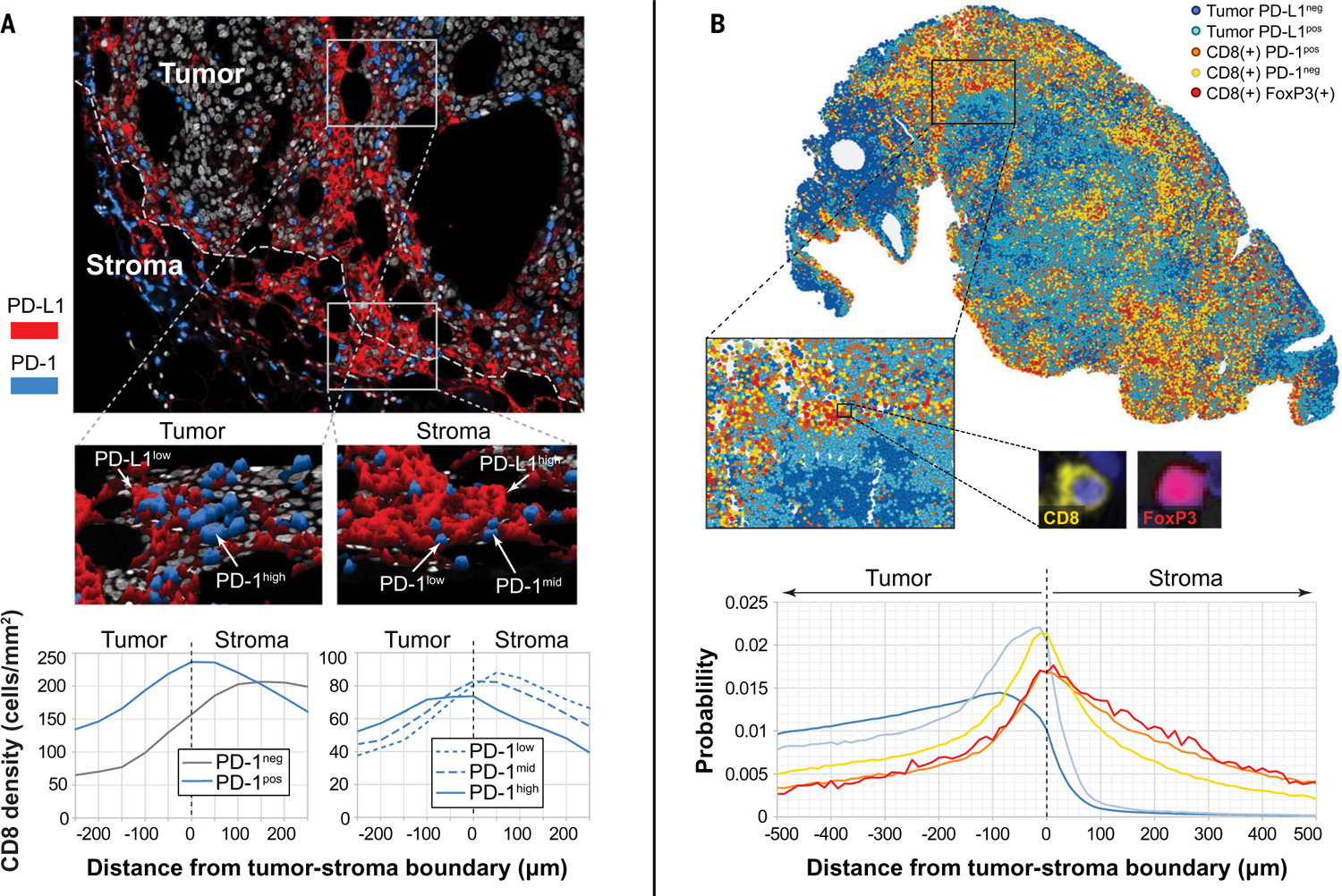
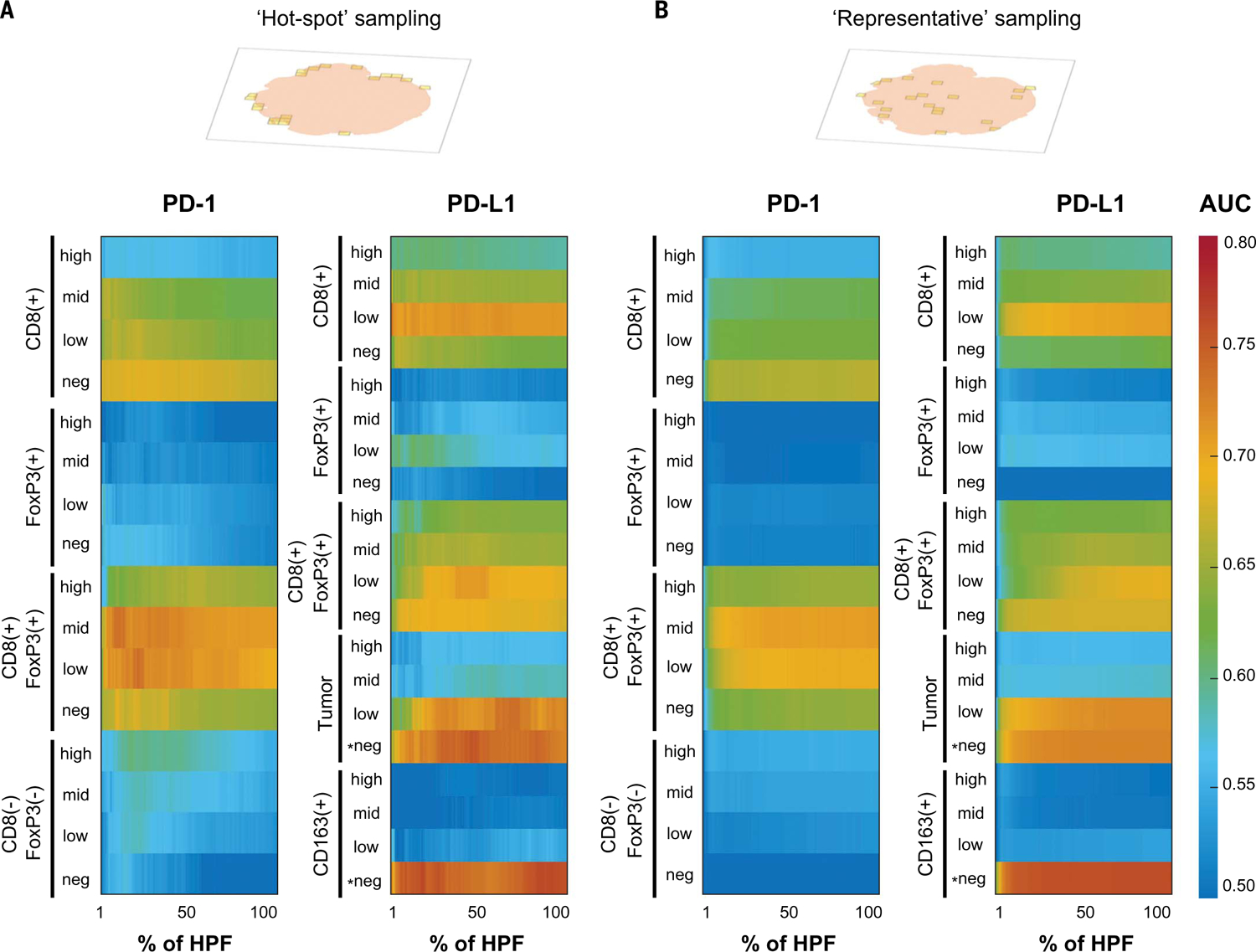
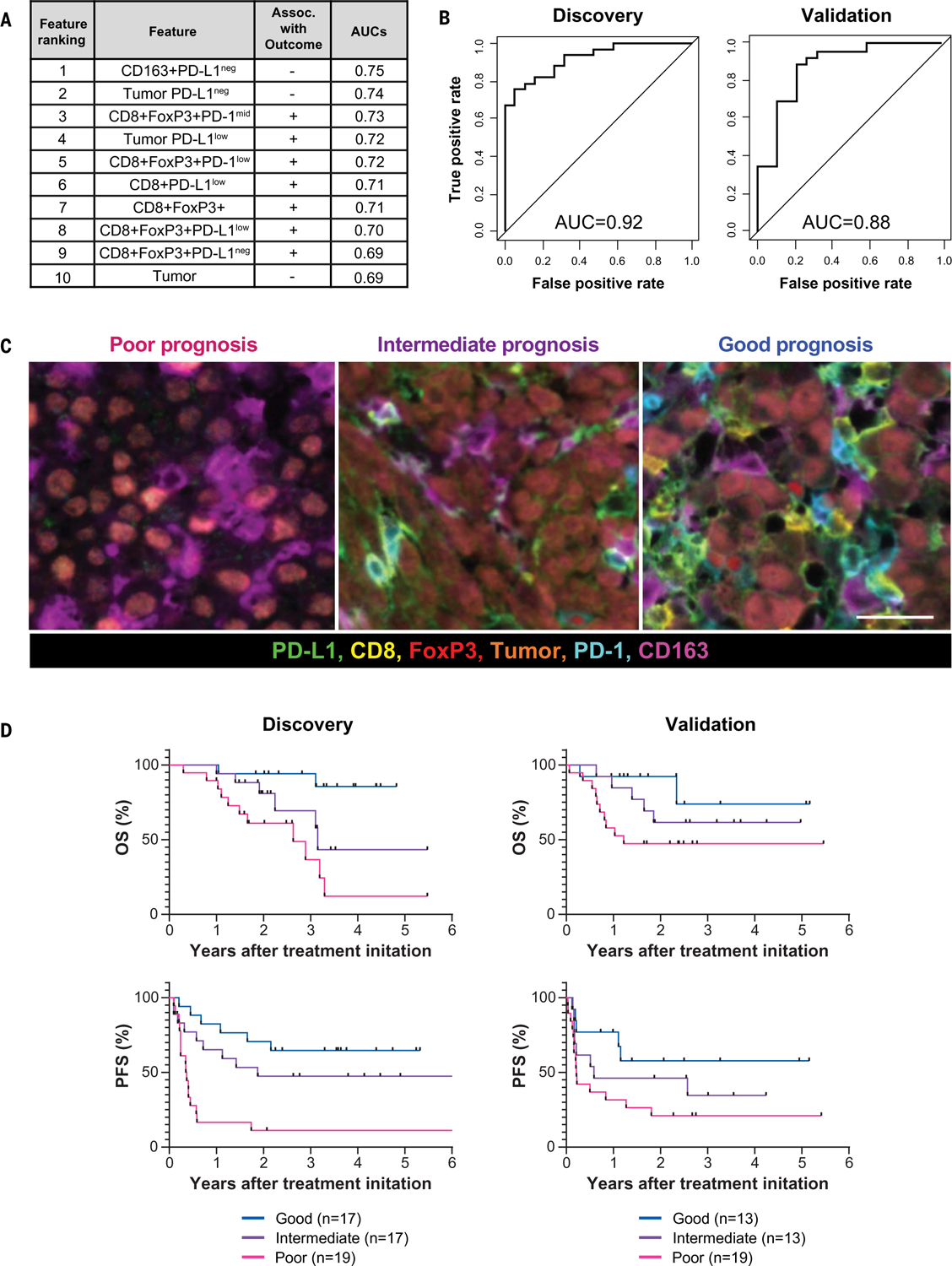
Next-generation tissue-based biomarkers for immunotherapy will likely include the simultaneous analysis of multiple cell types and their spatial interactions, as well as distinct expression patterns of immunoregulatory molecules. Here, we introduce a comprehensive platform for multispectral imaging and mapping of multiple parameters in tumor tissue sections with high-fidelity single-cell resolution. Image analysis and data handling components were drawn from the field of astronomy. Using this "AstroPath" whole-slide platform and only six markers, we identified key features in pretreatment melanoma specimens that predicted response to anti-programmed cell death-1 (PD-1)-based therapy, including CD163+PD-L1- myeloid cells and CD8+FoxP3+PD-1low/mid T cells. These features were combined to stratify long-term survival after anti-PD-1 blockade. This signature was validated in an independent cohort of patients with melanoma from a different institution.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures
Comment in
-
Multiplex computational pathology for treatment response predication.Cancer Cell. 2021 Aug 9;39(8):1053-1055. doi: 10.1016/j.ccell.2021.07.014. Cancer Cell. 2021. PMID: 34375608
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
