

High-throughput quantitation of SARS-CoV-2 antibodies in a single-dilution homogeneous assay
- PMID: 34112850
- PMCID: PMC8192771
- DOI: 10.1038/s41598-021-91300-5
High-throughput quantitation of SARS-CoV-2 antibodies in a single-dilution homogeneous assay
Abstract
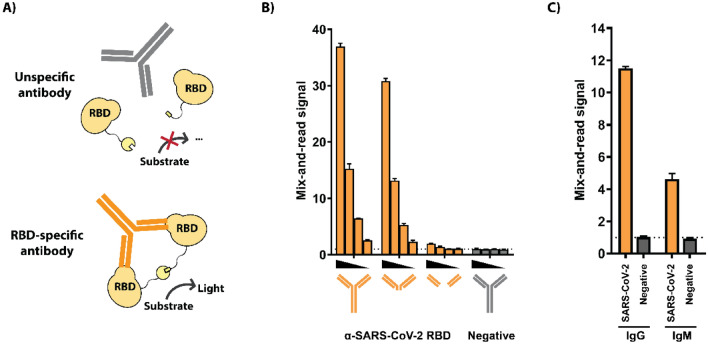
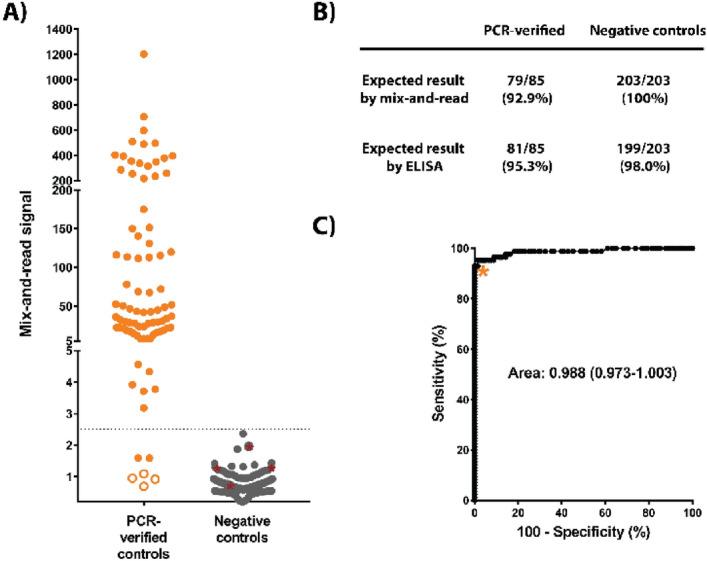
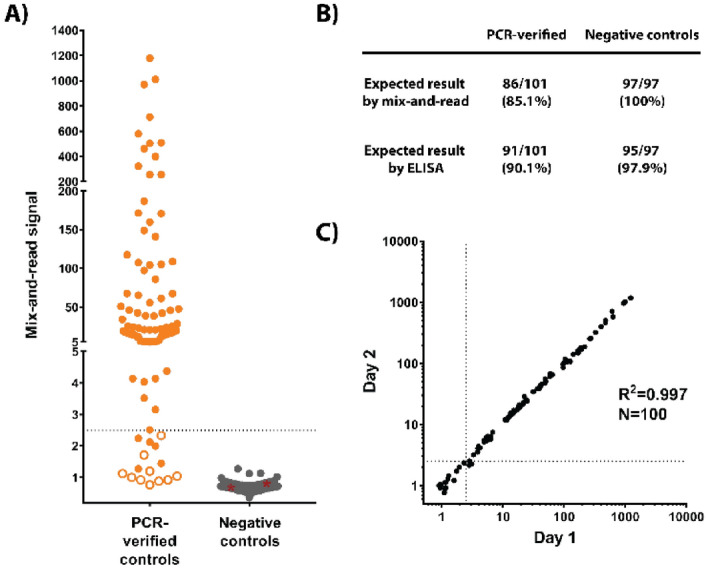
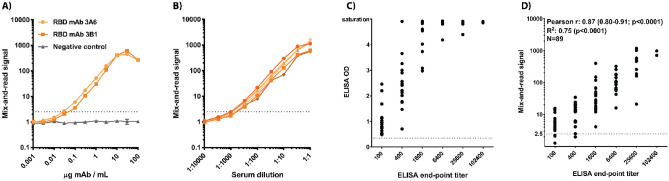
SARS-CoV-2 emerged in late 2019 and has since spread around the world, causing a pandemic of the respiratory disease COVID-19. Detecting antibodies against the virus is an essential tool for tracking infections and developing vaccines. Such tests, primarily utilizing the enzyme-linked immunosorbent assay (ELISA) principle, can be either qualitative (reporting positive/negative results) or quantitative (reporting a value representing the quantity of specific antibodies). Quantitation is vital for determining stability or decline of antibody titers in convalescence, efficacy of different vaccination regimens, and detection of asymptomatic infections. Quantitation typically requires two-step ELISA testing, in which samples are first screened in a qualitative assay and positive samples are subsequently analyzed as a dilution series. To overcome the throughput limitations of this approach, we developed a simpler and faster system that is highly automatable and achieves quantitation in a single-dilution screening format with sensitivity and specificity comparable to those of ELISA.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- WHO. WHO Statement Regarding Cluster of Pneumonia Cases In Wuhan, China. Available at: https://www.who.int/china/news/detail/09-01-2020-who-statement-regarding... (2020).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
