

The predictive ability of the 313 variant-based polygenic risk score for contralateral breast cancer risk prediction in women of European ancestry with a heterozygous BRCA1 or BRCA2 pathogenic variant
- PMID: 34113011
- PMCID: PMC8460445
- DOI: 10.1038/s41436-021-01198-7
The predictive ability of the 313 variant-based polygenic risk score for contralateral breast cancer risk prediction in women of European ancestry with a heterozygous BRCA1 or BRCA2 pathogenic variant
Abstract
Purpose: To evaluate the association between a previously published 313 variant-based breast cancer (BC) polygenic risk score (PRS313) and contralateral breast cancer (CBC) risk, in BRCA1 and BRCA2 pathogenic variant heterozygotes.
Methods: We included women of European ancestry with a prevalent first primary invasive BC (BRCA1 = 6,591 with 1,402 prevalent CBC cases; BRCA2 = 4,208 with 647 prevalent CBC cases) from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA), a large international retrospective series. Cox regression analysis was performed to assess the association between overall and ER-specific PRS313 and CBC risk.
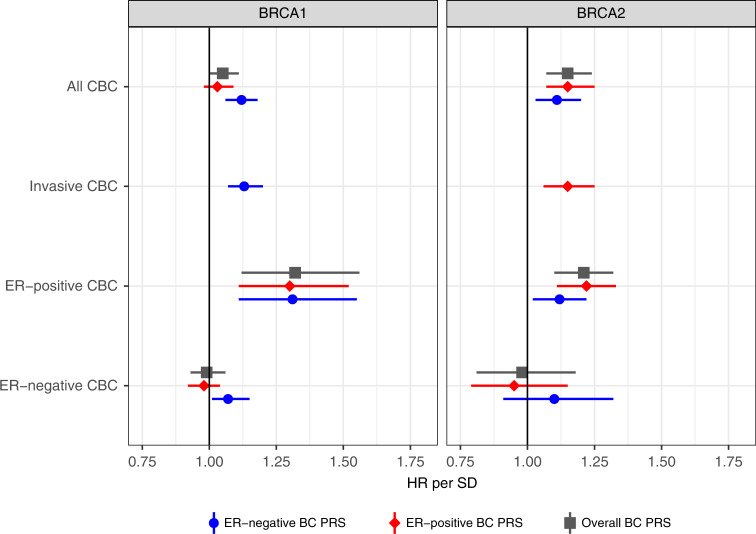
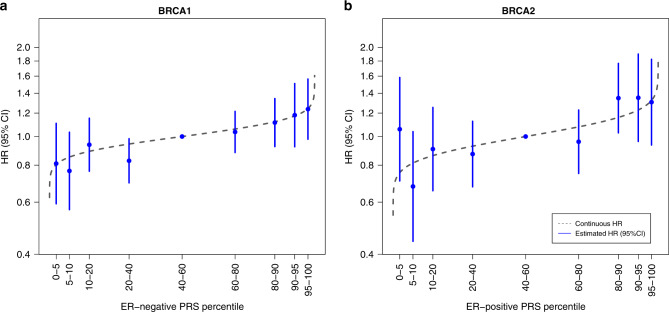
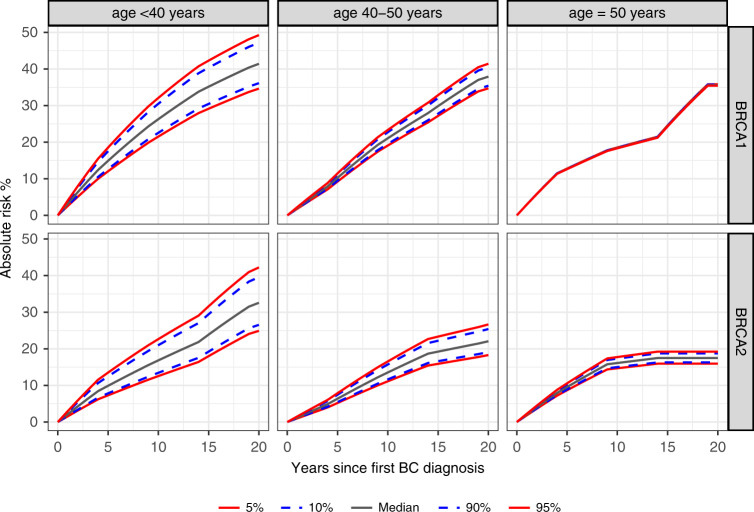
Results: For BRCA1 heterozygotes the estrogen receptor (ER)-negative PRS313 showed the largest association with CBC risk, hazard ratio (HR) per SD = 1.12, 95% confidence interval (CI) (1.06-1.18), C-index = 0.53; for BRCA2 heterozygotes, this was the ER-positive PRS313, HR = 1.15, 95% CI (1.07-1.25), C-index = 0.57. Adjusting for family history, age at diagnosis, treatment, or pathological characteristics for the first BC did not change association effect sizes. For women developing first BC < age 40 years, the cumulative PRS313 5th and 95th percentile 10-year CBC risks were 22% and 32% for BRCA1 and 13% and 23% for BRCA2 heterozygotes, respectively.
Conclusion: The PRS313 can be used to refine individual CBC risks for BRCA1/2 heterozygotes of European ancestry, however the PRS313 needs to be considered in the context of a multifactorial risk model to evaluate whether it might influence clinical decision-making.
© 2021. The Author(s).
Conflict of interest statement
C. Isaacs is consultant to Astra Zeneca, Novartis, Pfizer, Genentech, PUMA, Seattle Genetics, and received research support from Tesaro. The other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000124/TR/NCATS NIH HHS/United States
- 203477/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- R01 CA214545/CA/NCI NIH HHS/United States
- 11174/CRUK_/Cancer Research UK/United Kingdom
- UL1 TR001863/TR/NCATS NIH HHS/United States
- C1287/A16563/CRUK_/Cancer Research UK/United Kingdom
- P30 CA168524/CA/NCI NIH HHS/United States
- C5047/A10692/CRUK_/Cancer Research UK/United Kingdom
- A11174/CRUK_/Cancer Research UK/United Kingdom
- C5047/A8384/CRUK_/Cancer Research UK/United Kingdom
- P30 CA008748/CA/NCI NIH HHS/United States
- C1287/A 10710/CRUK_/Cancer Research UK/United Kingdom
- U19 CA148065/CA/NCI NIH HHS/United States
- RC4 CA153828/CA/NCI NIH HHS/United States
- C1281/A12014/CRUK_/Cancer Research UK/United Kingdom
- C12292/A2086/CRUK_/Cancer Research UK/United Kingdom
- 23382/CRUK_/Cancer Research UK/United Kingdom
- C12292/A11174/CRUK_/Cancer Research UK/United Kingdom
- DH_/Department of Health/United Kingdom
- 20861/CRUK_/Cancer Research UK/United Kingdom
- 26886/CRUK_/Cancer Research UK/United Kingdom
- P20 GM130423/GM/NIGMS NIH HHS/United States
- U10 CA180822/CA/NCI NIH HHS/United States
- C5047/A15007/CRUK_/Cancer Research UK/United Kingdom
- UM1 CA164920/CA/NCI NIH HHS/United States
- U10 CA180868/CA/NCI NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- C8197/A16565/CRUK_/Cancer Research UK/United Kingdom
- 10118/CRUK_/Cancer Research UK/United Kingdom
- R01 CA192393/CA/NCI NIH HHS/United States
- C1287/A10118/CRUK_/Cancer Research UK/United Kingdom
- R25 CA112486/CA/NCI NIH HHS/United States
