

Prediction of ventricular arrhythmia in phospholamban p.Arg14del mutation carriers-reaching the frontiers of individual risk prediction
- PMID: 34113975
- PMCID: PMC8325776
- DOI: 10.1093/eurheartj/ehab294
Prediction of ventricular arrhythmia in phospholamban p.Arg14del mutation carriers-reaching the frontiers of individual risk prediction
Abstract
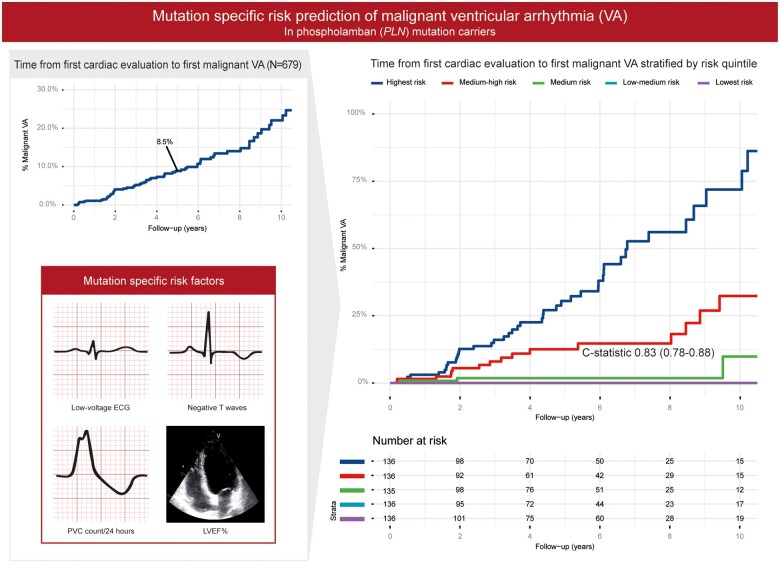
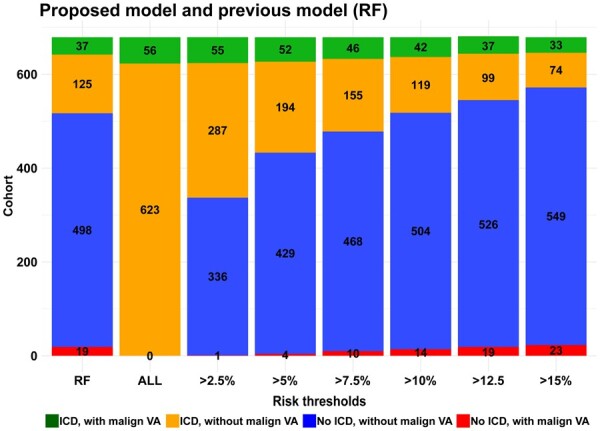
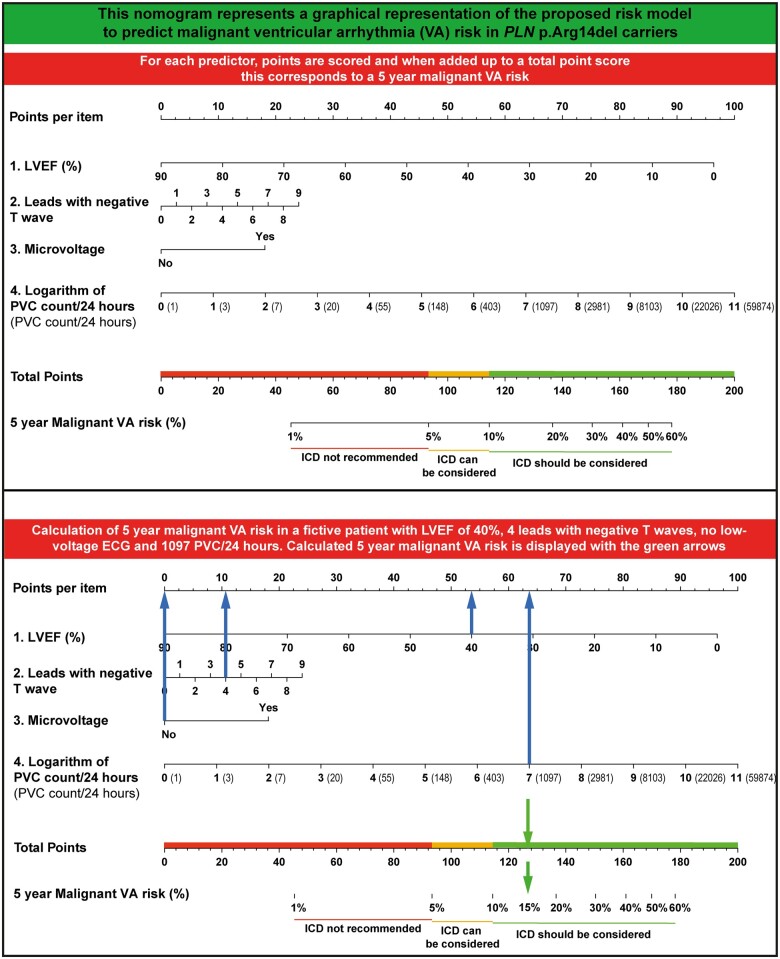
Aims: This study aims to improve risk stratification for primary prevention implantable cardioverter defibrillator (ICD) implantation by developing a new mutation-specific prediction model for malignant ventricular arrhythmia (VA) in phospholamban (PLN) p.Arg14del mutation carriers. The proposed model is compared to an existing PLN risk model.
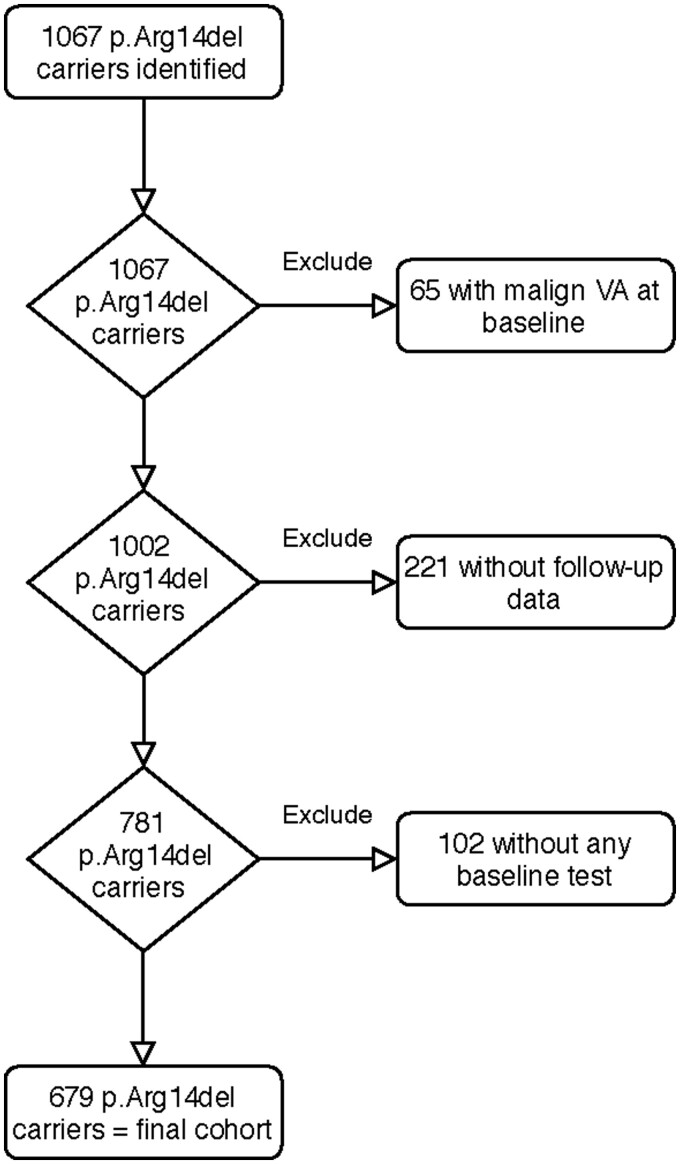
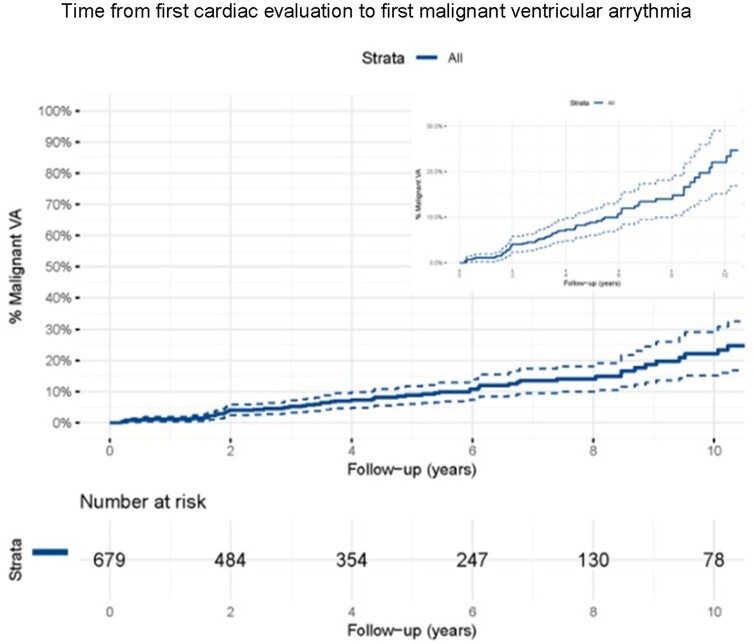
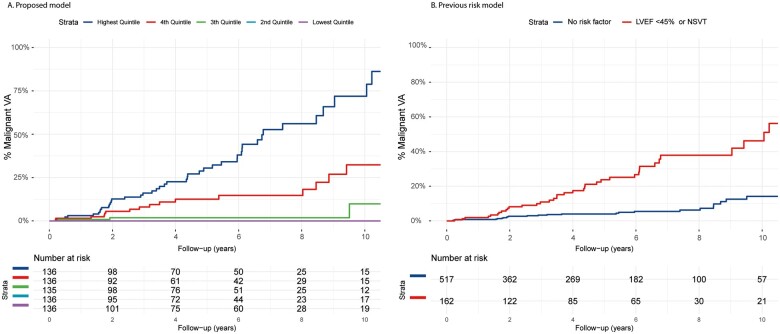
Methods and results: Data were collected from PLN p.Arg14del mutation carriers with no history of malignant VA at baseline, identified between 2009 and 2020. Malignant VA was defined as sustained VA, appropriate ICD intervention, or (aborted) sudden cardiac death. A prediction model was developed using Cox regression. The study cohort consisted of 679 PLN p.Arg14del mutation carriers, with a minority of index patients (17%) and male sex (43%), and a median age of 42 years [interquartile range (IQR) 27-55]. During a median follow-up of 4.3 years (IQR 1.7-7.4), 72 (10.6%) carriers experienced malignant VA. Significant predictors were left ventricular ejection fraction, premature ventricular contraction count/24 h, amount of negative T waves, and presence of low-voltage electrocardiogram. The multivariable model had an excellent discriminative ability {C-statistic 0.83 [95% confidence interval (CI) 0.78-0.88]}. Applying the existing PLN risk model to the complete cohort yielded a C-statistic of 0.68 (95% CI 0.61-0.75).
Conclusion: This new mutation-specific prediction model for individual VA risk in PLN p.Arg14del mutation carriers is superior to the existing PLN risk model, suggesting that risk prediction using mutation-specific phenotypic features can improve accuracy compared to a more generic approach.
Keywords: Cardiomyopathy; Implantable cardioverter defibrillator; Phospholamban; Risk stratification; Sudden cardiac death.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Arrhythmic risk stratification in arrhythmogenic cardiomyopathy: new predictors for left-sided variants?Eur Heart J. 2021 Jul 31;42(29):2851-2853. doi: 10.1093/eurheartj/ehab355. Eur Heart J. 2021. PMID: 34151346 No abstract available.
References
-
- Haghighi K, Kolokathis F, Pater L, Lynch RA, Asahi M, Gramolini AO, Fan GC, Tsiapras D, Hahn HS, Adamopoulos S, Liggett SB, Dorn GW 2nd, MacLennan DH, Kremastinos DT, Kranias EG. Human phospholamban null results in lethal dilated cardiomyopathy revealing a critical difference between mouse and human. J Clin Invest 2003;111:869–876. - PMC - PubMed
-
- Haghighi K, Kolokathis F, Gramolini AO, Waggoner JR, Pater L, Lynch RA, Fan GC, Tsiapras D, Parekh RR, Dorn GW 2nd, MacLennan DH, Kremastinos DT, Kranias EG. A mutation in the human phospholamban gene, deleting arginine 14, results in lethal, hereditary cardiomyopathy. Proc Natl Acad Sci U S A 2006;103:1388–1393. - PMC - PubMed
-
- Medeiros A, Biagi DG, Sobreira TJ, de Oliveira PS, Negrao CE, Mansur AJ, Krieger JE, Brum PC, Pereira AC. Mutations in the human phospholamban gene in patients with heart failure. Am Heart J 2011;162:1088–1095.e1. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
