

Renal function in patients with significant tricuspid regurgitation: pathophysiological mechanisms and prognostic implications
- PMID: 34114700
- PMCID: PMC8453518
- DOI: 10.1111/joim.13312
Renal function in patients with significant tricuspid regurgitation: pathophysiological mechanisms and prognostic implications
Abstract
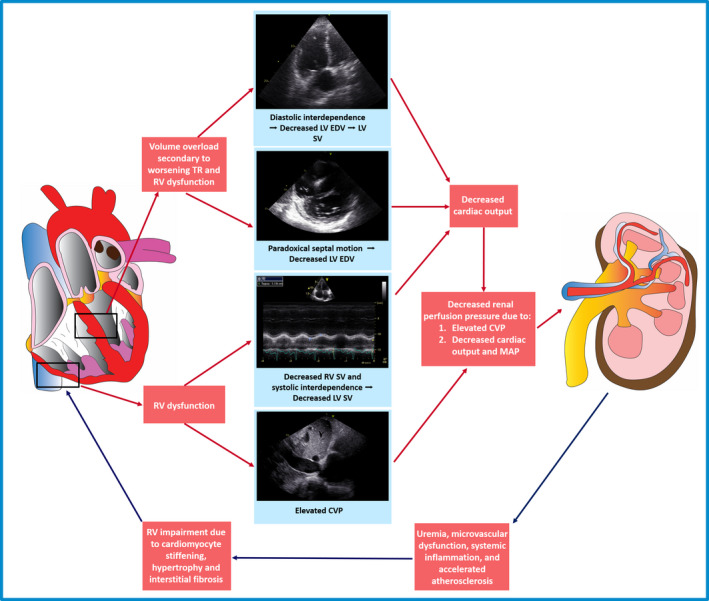
Background: The pathophysiological mechanisms linking tricuspid regurgitation (TR) and chronic kidney disease (CKD) remain unknown. This study aimed to determine which pathophysiological mechanisms related to TR are independently associated with renal dysfunction and to evaluate the impact of renal impairment on long-term prognosis in patients with significant (≥ moderate) secondary TR.
Methods: A total of 1234 individuals (72 [IQR 63-78] years, 50% male) with significant secondary TR were followed up for the occurrence of all-cause mortality and the presence of significant renal impairment (eGFR of <60 mL min-1 1.73 m-2 ) at the time of baseline echocardiography.
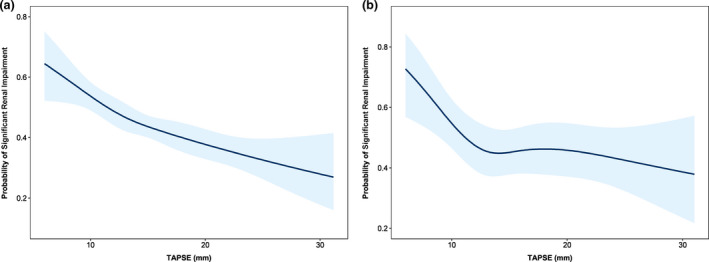
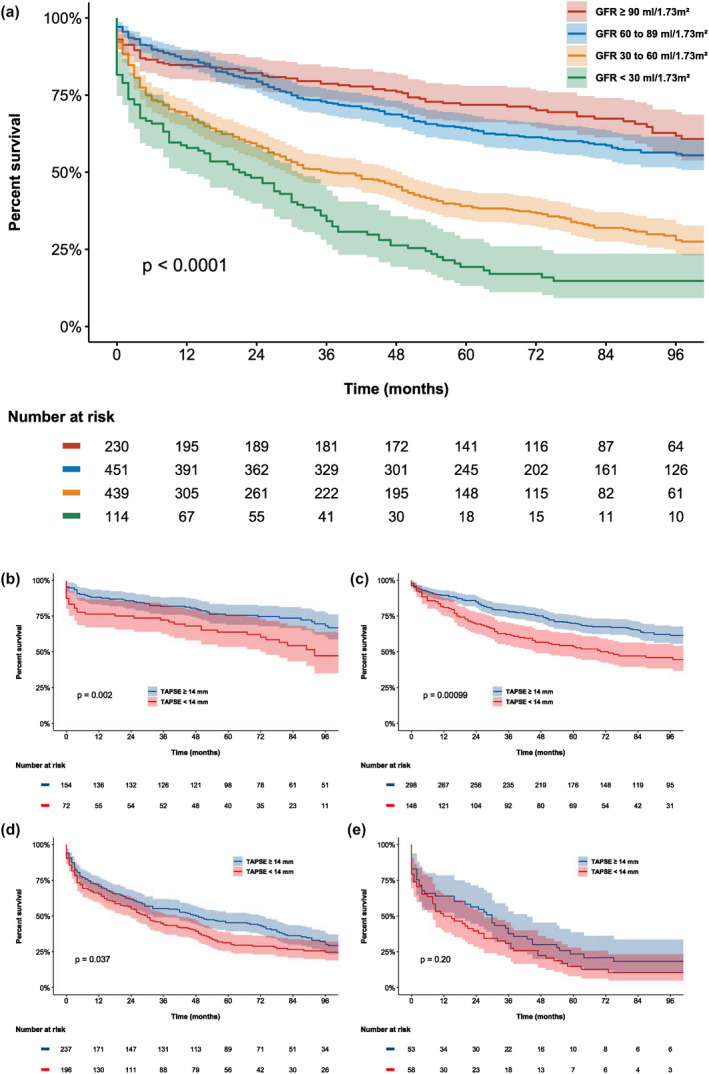
Results: Multivariable analysis demonstrated that severe right ventricular (RV) dysfunction (TAPSE < 14 mm) was independently associated with the presence of significant renal impairment (OR 1.49, 95% CI 1.11 to 1.99, P = 0.008). Worse renal function was associated with a significant reduction in survival at 1 and 5 years (85% vs. 87% vs. 68% vs. 58% at 1 year, and 72% vs. 64% vs. 39% vs. 19% at 5 years, for stage 1, 2, 3 and 4-5 CKD groups, respectively, P < 0.001). The presence of severe RV dysfunction was associated with reduced overall survival in stage 1-3 CKD groups, but not in stage 4-5 CKD groups.
Conclusions: Of the pathophysiological mechanisms identified by echocardiography that are associated with significant secondary TR, only severe RV dysfunction was independently associated with the presence of significant renal impairment. In addition, worse renal function according to CKD group was associated with a significant reduction in survival.
Keywords: chronic kidney disease; renal dysfunction; right ventricular dysfunction; tricuspid regurgitation.
© 2021 The Association for the Publication of the Journal of Internal Medicine.
Conflict of interest statement
The Department of Cardiology of the Leiden University Medical Center received research grants from Abbott Vascular, Bayer, BioVentrix, Medtronic, Biotronik, Boston Scientific, GE Healthcare and Edwards Lifesciences. Jeroen Bax and Nina Ajmone Marsan received speaking fees from Abbott Vascular. Victoria Delgado received speaker fees from Abbott Vascular, Medtronic, Edwards Lifesciences, MSD and GE Healthcare. The remaining authors have nothing to disclose.
Figures
References
-
- Badano LP, Muraru D, Enriquez‐Sarano M. Assessment of functional tricuspid regurgitation. Eur Heart J. 2013;34:1875–85. - PubMed
-
- Benfari G, Antoine C, Miller WL, et al. Excess mortality associated with functional tricuspid regurgitation complicating heart failure with reduced ejection fraction. Circulation. 2019;140:196–206. - PubMed
-
- Bar N, Schwartz LA, Biner S, et al. Clinical outcome of isolated tricuspid regurgitation in patients with preserved left ventricular ejection fraction and pulmonary hypertension. J Am Soc Echocardiogr. 2018;31:34–41. - PubMed
-
- Taramasso M, Benfari G, van der Bijl P, et al. Transcatheter versus medical treatment of patients with symptomatic severe tricuspid regurgitation. J Am Coll Cardiol. 2019;74:2998–3008. - PubMed
-
- Maeder MT, Holst DP, Kaye DM. Tricuspid regurgitation contributes to renal dysfunction in patients with heart failure. J Card Fail. 2008;14:824–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
