

The comparison of Nice knots and traditional methods as an auxiliary reduction-fixation technique in pre-contoured locking plate fixation for comminuted Robinson type 2B clavicle fracture: A retrospective study
- PMID: 34115029
- PMCID: PMC8202591
- DOI: 10.1097/MD.0000000000026282
The comparison of Nice knots and traditional methods as an auxiliary reduction-fixation technique in pre-contoured locking plate fixation for comminuted Robinson type 2B clavicle fracture: A retrospective study
Abstract
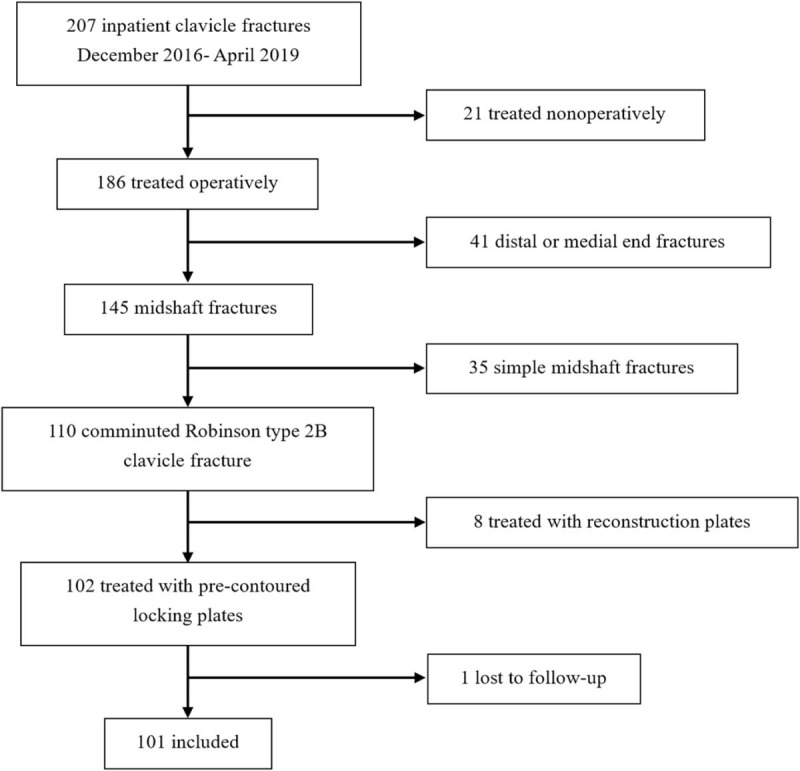
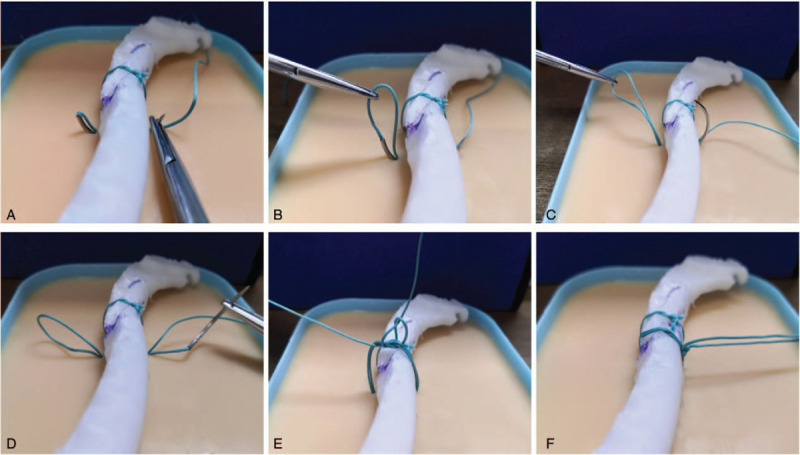
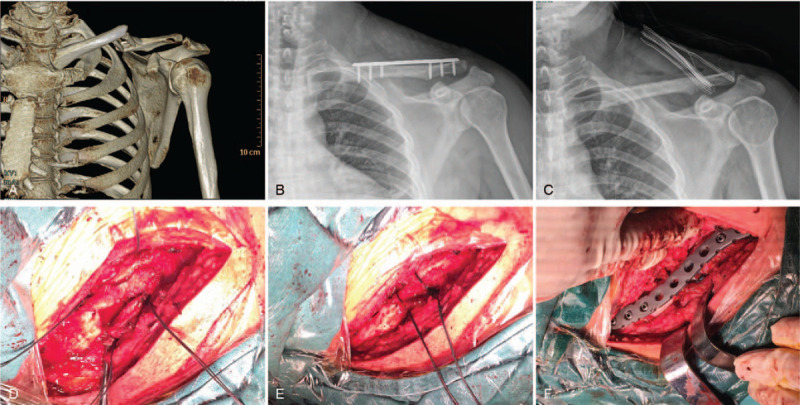
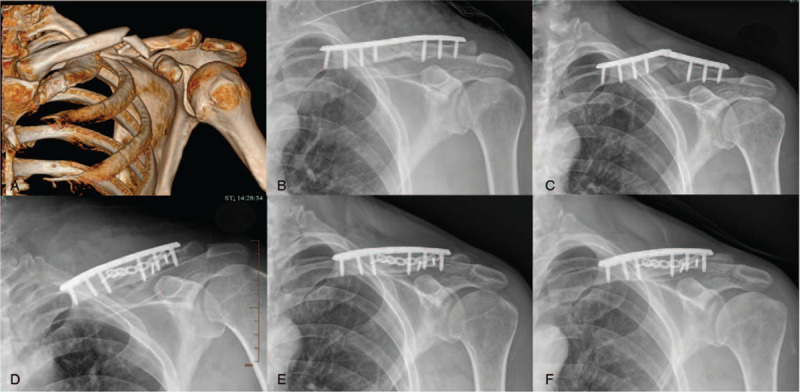
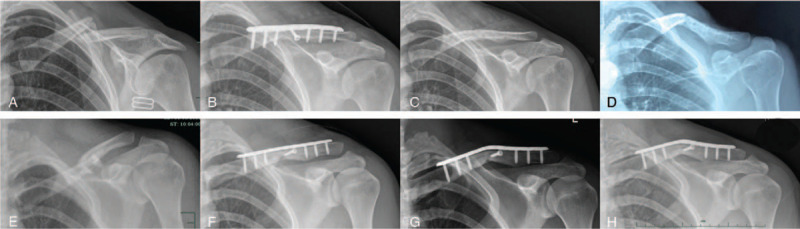
Open reduction and pre-contoured locking plate fixation is a popular treatment option for displaced midshaft clavicle fracture. Lag screw and cerclage are 2 main intraoperative techniques to reduce and fix fragments. However, both lag screw and metallic cerclage have disadvantages. The doubled-suture Nice knot has been reported in many areas of orthopedic surgery for its effectiveness. This study aims to compare the outcomes of comminuted mid-shaft clavicle fractures reduced by Nice knots vs traditional techniques (lag screw or/and metallic cerclage) when bridged with pre-contoured locking plates.We retrospectively reviewed 101 patients (65 females and 36 males) diagnosed with midshaft clavicle fractures with at least one wedge fragment reduced by either Nice knots or traditional methods and bridged with pre-contoured locking plates between December 2016 and April 2019. Operation time, functional outcomes, pain, patient satisfaction, fracture healing, and complications were assessed at a follow-up of 12 to 40 months.The mean age of all the patients was 50.8 years. There were 52 and 49 patients in the Nice knot group and traditional group respectively, and no differences between 2 groups were found in general patient characteristics, fracture type, follow up and injury-to-surgery duration. The Nice knot group had significant less operation time (P < .01) than the traditional group (mean and standard deviation [SD], 78.6 ± 19.0 compared with 94.4 ± 29.9 minutes, respectively). For healing time, functional score, pain, satisfaction and complications, there were no significant differences between groups, despite the Nice knot group had slightly better results.Both Nice knots and traditional methods treated for comminuted Robinson type 2B clavicle fractures were effective and safe. And the Nice knots seemed to be superior with significant less operation time.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Khan LA, Bradnock TJ, Scott C, et al. . Fractures of the clavicle. J Bone Joint Surg Am 2009;91:447–60. - PubMed
-
- van der Meijden OA, Gaskill TR, Millett PJ. Treatment of clavicle fractures: current concepts review. J Shoulder Elbow Surg 2012;21:423–9. - PubMed
-
- Chen W, Zhu Y, Liu S, et al. . Demographic and socioeconomic factors influencing the incidence of clavicle fractures, a national population-based survey of five hundred and twelve thousand, one hundred and eighty seven individuals. Int Orthop 2018;42:651–8. - PubMed
-
- Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476–84. - PubMed
-
- Neer CS, 2nd. Nonunion of the clavicle. J Am Med Assoc 1960;172:1006–11. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
