

Clonal dynamics and clinical implications of postremission clonal hematopoiesis in acute myeloid leukemia
- PMID: 34115096
- PMCID: PMC8569418
- DOI: 10.1182/blood.2020010483
Clonal dynamics and clinical implications of postremission clonal hematopoiesis in acute myeloid leukemia
Abstract
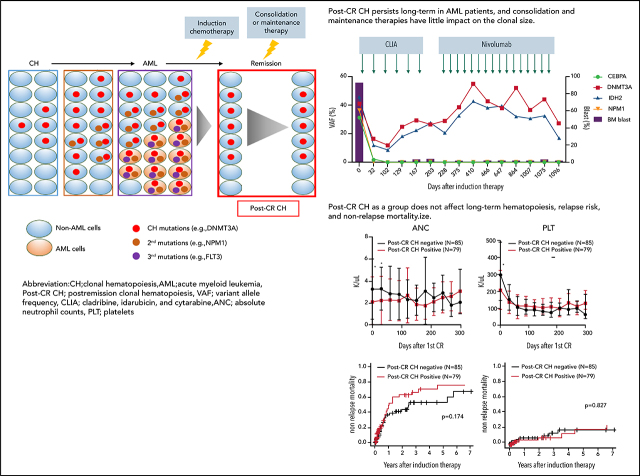
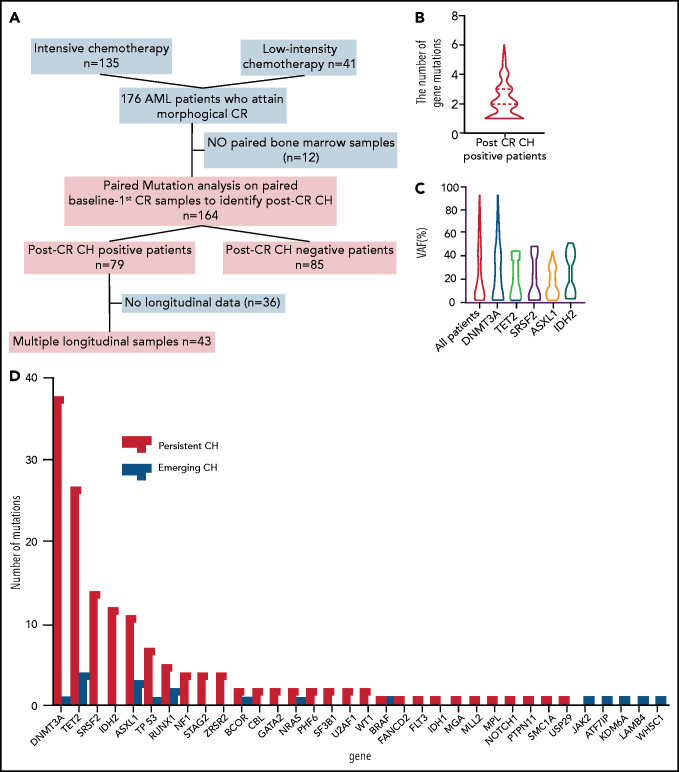
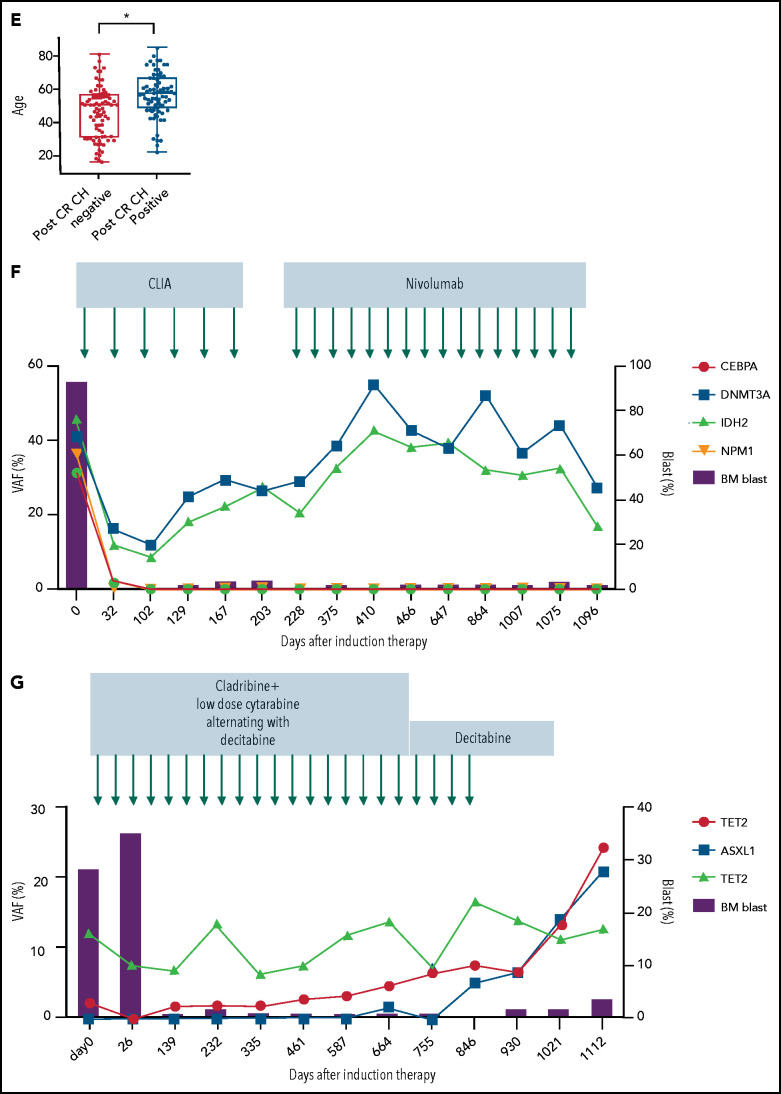
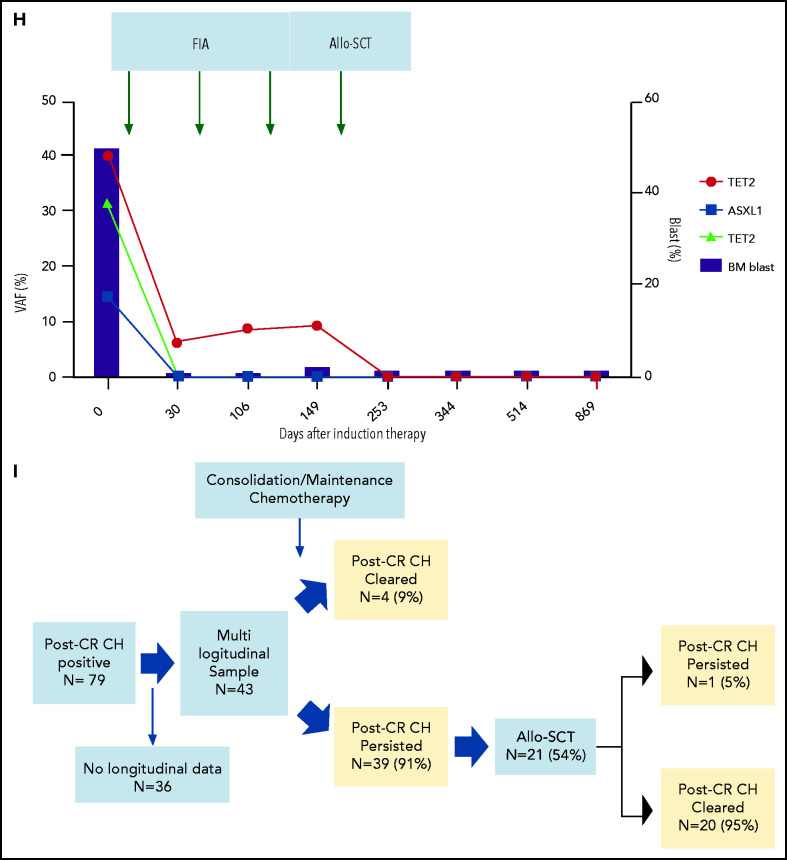
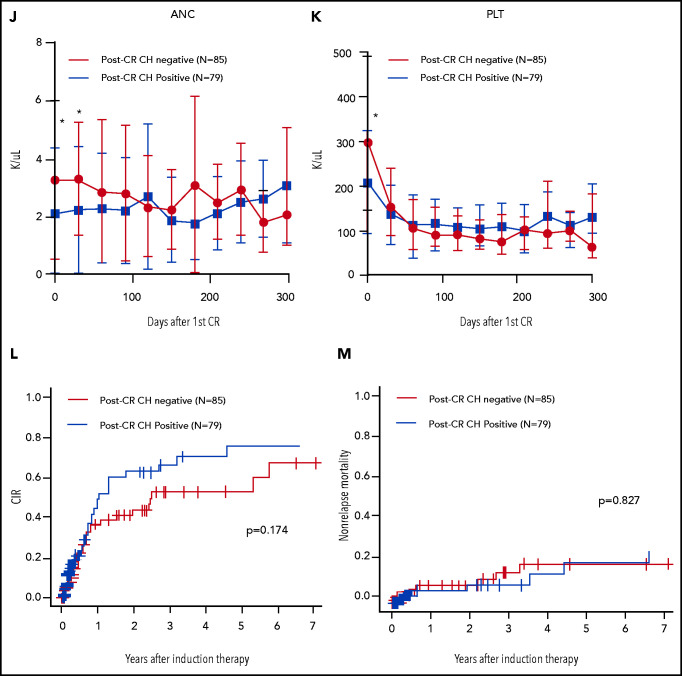
Although clonal hematopoiesis (CH) can precede the development of acute myeloid leukemia (AML), it can also persist after achieving remission. Long-term clonal dynamics and clinical implications of persistent CH are not well understood. Here, we studied the prevalence, dynamics, and clinical implications of postremission CH in 164 AML patients who attained complete remission after induction chemotherapies. Postremission CH was identified in 79 (48%) patients. Postremission CH persisted long term in 91% of the trackable patients despite treatment with various types of consolidation and maintenance therapies. Postremission CH was eradicated in 20 out of 21 (95%) patients who underwent allogeneic stem cell transplant. Although patients with postremission CH as a group had comparable hematopoiesis with those without it, patients with persistent TET2 mutations showed significant neutropenia long term. Postremission CH had little impact on relapse risk, nonrelapse mortality, and incidence of atherosclerotic cardiovascular disease, although the clinical impact of post-CR CH was heterogeneous among different mutations. These data suggest that although residual clonal hematopoietic stem cells are generally resistant to consolidation and maintenance therapies, they retain the ability to maintain normal hematopoiesis and have little impact on clinical outcomes. Larger study is needed to dissect the gene-specific heterogeneity.
© 2021 by The American Society of Hematology.
Figures
References
-
- Arends CM, Galan-Sousa J, Hoyer K, et al. . Hematopoietic lineage distribution and evolutionary dynamics of clonal hematopoiesis. Leukemia. 2018;32(9):1908-1919. - PubMed
-
- Jongen-Lavrencic M, Grob T, Hanekamp D, et al. . Molecular minimal residual disease in acute myeloid leukemia. N Engl J Med. 2018;378(13):1189-1199. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
