

International Analysis of Electronic Health Records of Children and Youth Hospitalized With COVID-19 Infection in 6 Countries
- PMID: 34115127
- PMCID: PMC8196345
- DOI: 10.1001/jamanetworkopen.2021.12596
International Analysis of Electronic Health Records of Children and Youth Hospitalized With COVID-19 Infection in 6 Countries
Erratum in
-
Errors in Byline.JAMA Netw Open. 2021 Jul 1;4(7):e2122388. doi: 10.1001/jamanetworkopen.2021.22388. JAMA Netw Open. 2021. PMID: 34297082 Free PMC article. No abstract available.
Abstract
Importance: Additional sources of pediatric epidemiological and clinical data are needed to efficiently study COVID-19 in children and youth and inform infection prevention and clinical treatment of pediatric patients.
Objective: To describe international hospitalization trends and key epidemiological and clinical features of children and youth with COVID-19.
Design, setting, and participants: This retrospective cohort study included pediatric patients hospitalized between February 2 and October 10, 2020. Patient-level electronic health record (EHR) data were collected across 27 hospitals in France, Germany, Spain, Singapore, the UK, and the US. Patients younger than 21 years who tested positive for COVID-19 and were hospitalized at an institution participating in the Consortium for Clinical Characterization of COVID-19 by EHR were included in the study.
Main outcomes and measures: Patient characteristics, clinical features, and medication use.
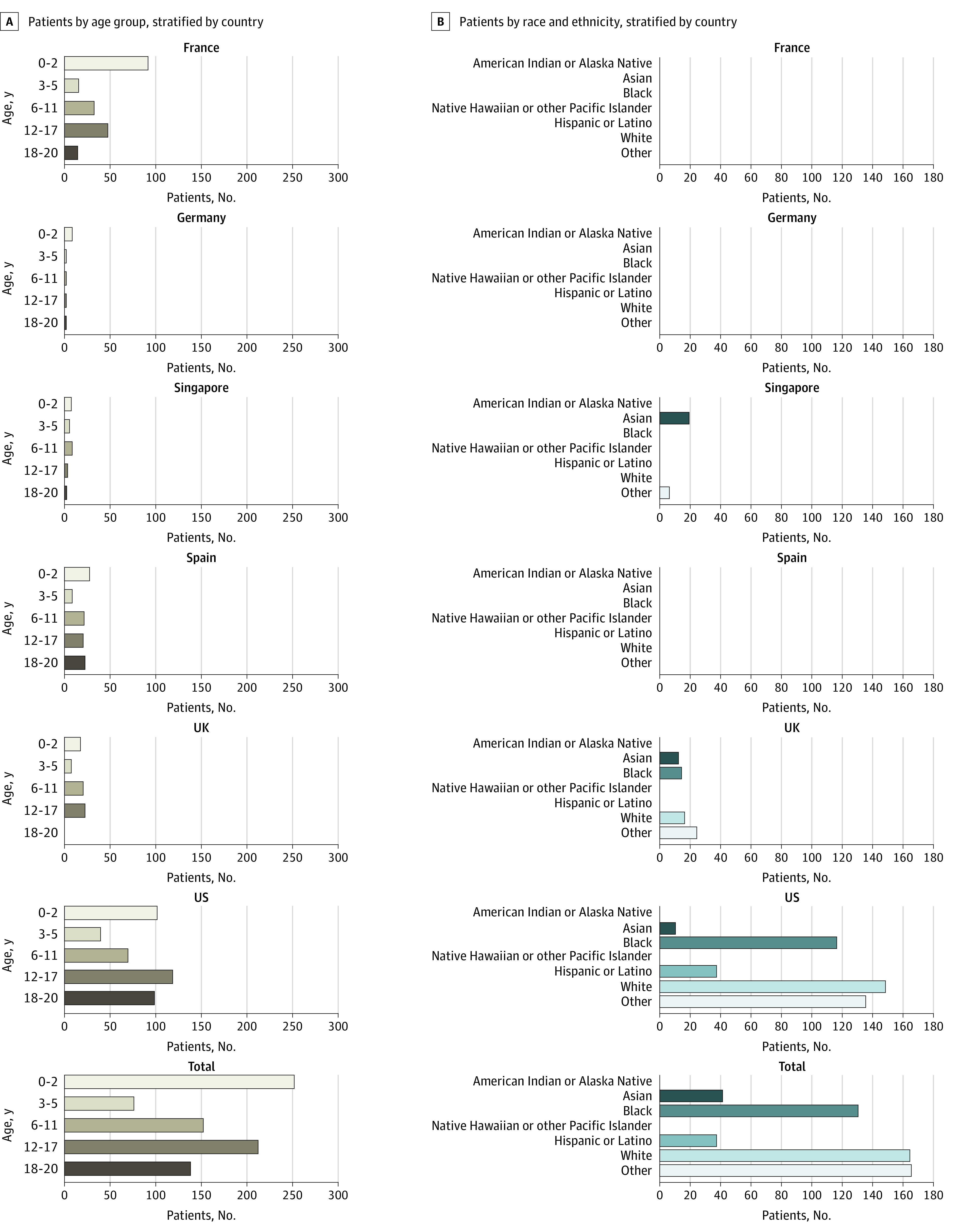
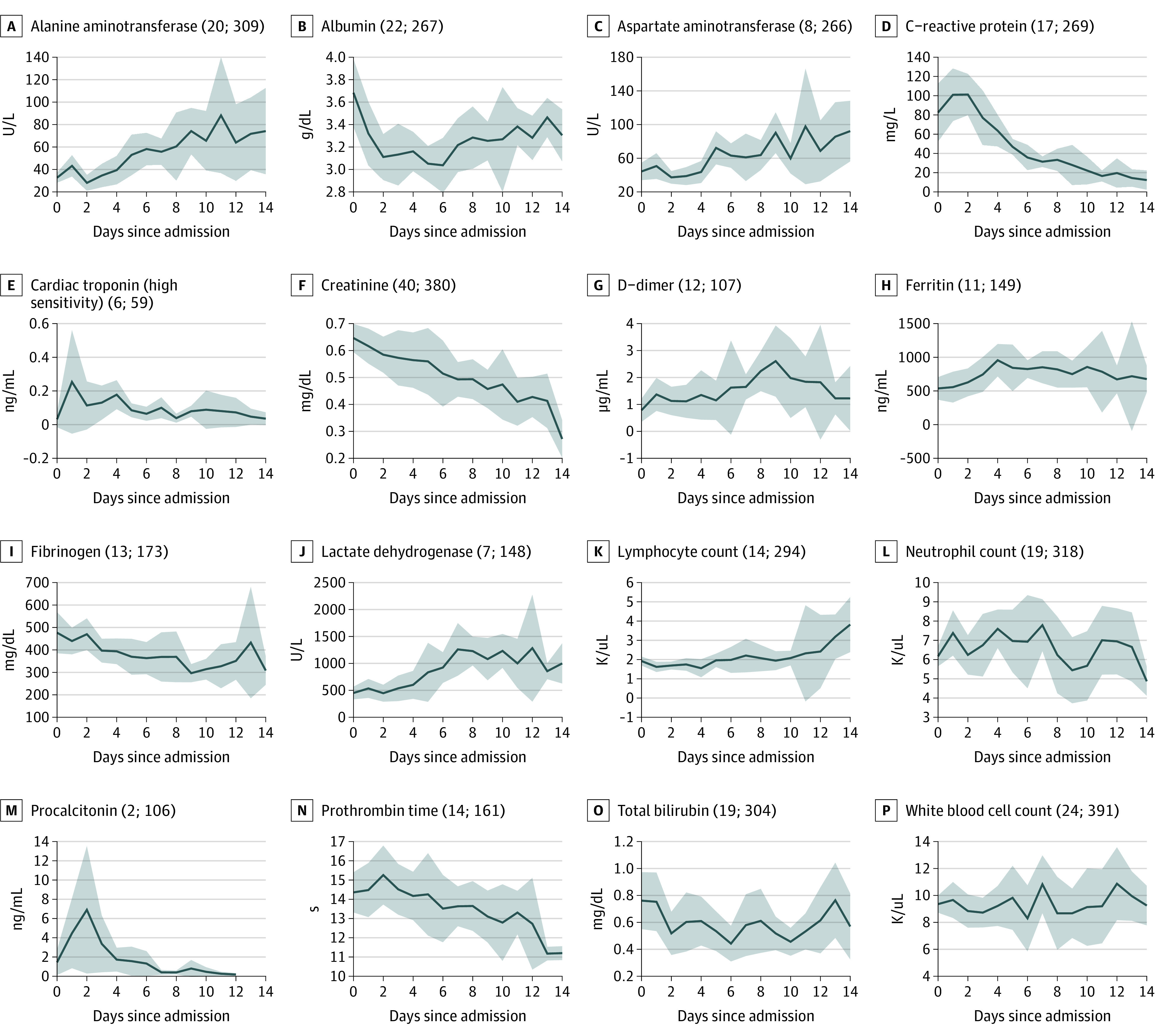
Results: There were 347 males (52%; 95% CI, 48.5-55.3) and 324 females (48%; 95% CI, 44.4-51.3) in this study's cohort. There was a bimodal age distribution, with the greatest proportion of patients in the 0- to 2-year (199 patients [30%]) and 12- to 17-year (170 patients [25%]) age range. Trends in hospitalizations for 671 children and youth found discrete surges with variable timing across 6 countries. Data from this cohort mirrored national-level pediatric hospitalization trends for most countries with available data, with peaks in hospitalizations during the initial spring surge occurring within 23 days in the national-level and 4CE data. A total of 27 364 laboratory values for 16 laboratory tests were analyzed, with mean values indicating elevations in markers of inflammation (C-reactive protein, 83 mg/L; 95% CI, 53-112 mg/L; ferritin, 417 ng/mL; 95% CI, 228-607 ng/mL; and procalcitonin, 1.45 ng/mL; 95% CI, 0.13-2.77 ng/mL). Abnormalities in coagulation were also evident (D-dimer, 0.78 ug/mL; 95% CI, 0.35-1.21 ug/mL; and fibrinogen, 477 mg/dL; 95% CI, 385-569 mg/dL). Cardiac troponin, when checked (n = 59), was elevated (0.032 ng/mL; 95% CI, 0.000-0.080 ng/mL). Common complications included cardiac arrhythmias (15.0%; 95% CI, 8.1%-21.7%), viral pneumonia (13.3%; 95% CI, 6.5%-20.1%), and respiratory failure (10.5%; 95% CI, 5.8%-15.3%). Few children were treated with COVID-19-directed medications.
Conclusions and relevance: This study of EHRs of children and youth hospitalized for COVID-19 in 6 countries demonstrated variability in hospitalization trends across countries and identified common complications and laboratory abnormalities in children and youth with COVID-19 infection. Large-scale informatics-based approaches to integrate and analyze data across health care systems complement methods of disease surveillance and advance understanding of epidemiological and clinical features associated with COVID-19 in children and youth.
Conflict of interest statement
Figures

Comment in
-
On the Usage of Combined Data Structures to Study COVID-19 in Understudied Populations.JAMA Netw Open. 2021 Jun 1;4(6):e2112874. doi: 10.1001/jamanetworkopen.2021.12874. JAMA Netw Open. 2021. PMID: 34115132 No abstract available.
References
Publication types
MeSH terms
Grants and funding
- T15 LM007092/LM/NLM NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- R01 NS098023/NS/NINDS NIH HHS/United States
- U24 HL148865/HL/NHLBI NIH HHS/United States
- T32 HG002295/HG/NHGRI NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- UL1 TR002366/TR/NCATS NIH HHS/United States
- FS/19/52/34563/BHF_/British Heart Foundation/United Kingdom
- R01 LM013337/LM/NLM NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- K12 HD047349/HD/NICHD NIH HHS/United States
- R01 HG009174/HG/NHGRI NIH HHS/United States
- T32 LM012203/LM/NLM NIH HHS/United States
- R01 LM013345/LM/NLM NIH HHS/United States
- UL1 TR002541/TR/NCATS NIH HHS/United States
- MC_PC_18034/MRC_/Medical Research Council/United Kingdom
- K23 HL148394/HL/NHLBI NIH HHS/United States
- UL1 TR002240/TR/NCATS NIH HHS/United States
- L40 HL148910/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
