

Trends in Venous Thromboembolism Anticoagulation in Patients Hospitalized With COVID-19
- PMID: 34115129
- PMCID: PMC8196344
- DOI: 10.1001/jamanetworkopen.2021.11788
Trends in Venous Thromboembolism Anticoagulation in Patients Hospitalized With COVID-19
Abstract
Importance: Venous thromboembolism (VTE) is a common complication of COVID-19. It is not well understood how hospitals have managed VTE prevention and the effect of prevention strategies on mortality.
Objective: To characterize frequency, variation across hospitals, and change over time in VTE prophylaxis and treatment-dose anticoagulation in patients hospitalized for COVID-19, as well as the association of anticoagulation strategies with in-hospital and 60-day mortality.
Design, setting, and participants: This cohort study of adults hospitalized with COVID-19 used a pseudorandom sample from 30 US hospitals in the state of Michigan participating in a collaborative quality initiative. Data analyzed were from patients hospitalized between March 7, 2020, and June 17, 2020. Data were analyzed through March 2021.
Exposures: Nonadherence to VTE prophylaxis (defined as missing ≥2 days of VTE prophylaxis) and receipt of treatment-dose or prophylactic-dose anticoagulants vs no anticoagulation during hospitalization.
Main outcomes and measures: The effect of nonadherence and anticoagulation strategies on in-hospital and 60-day mortality was assessed using multinomial logit models with inverse probability of treatment weighting.
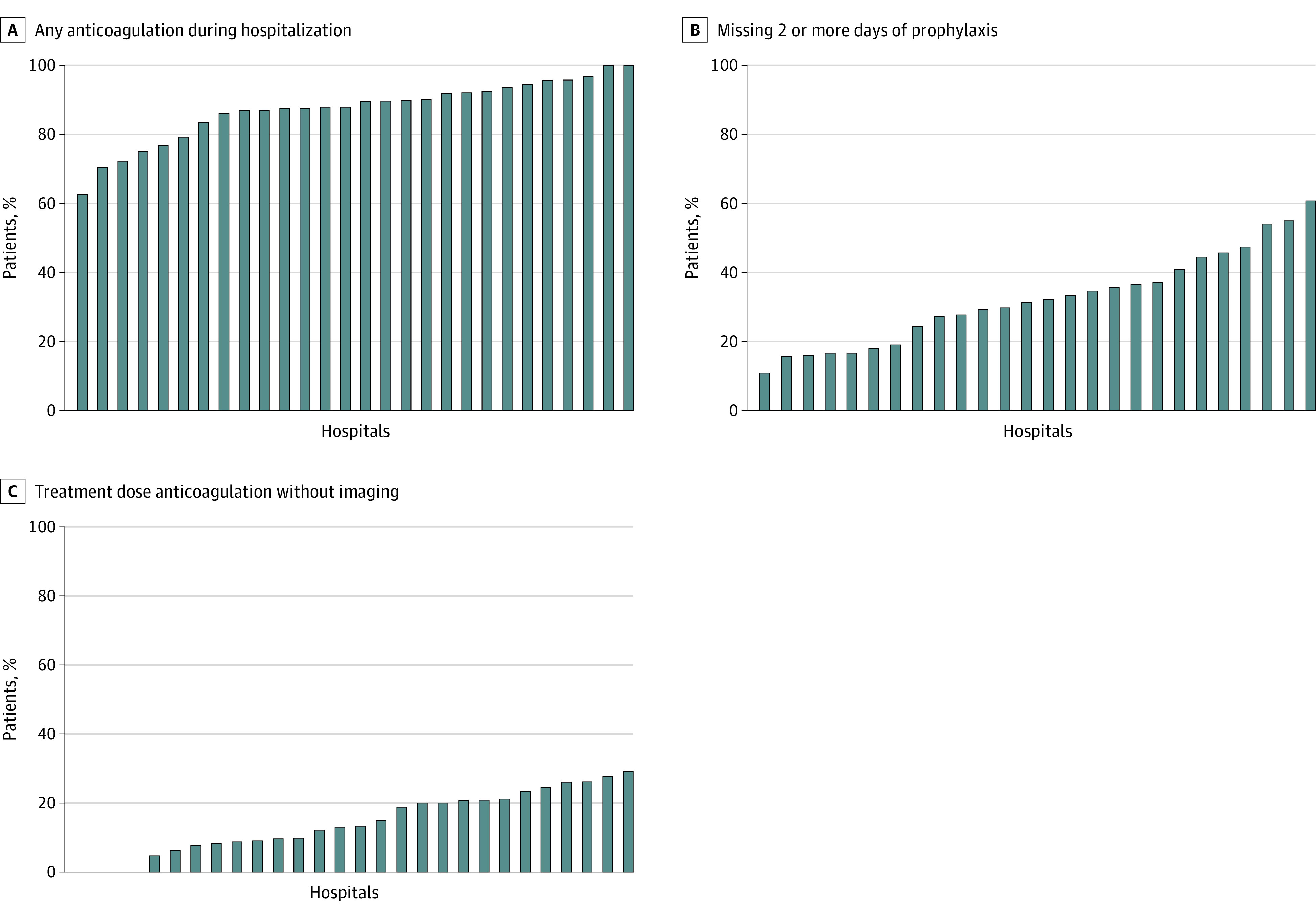
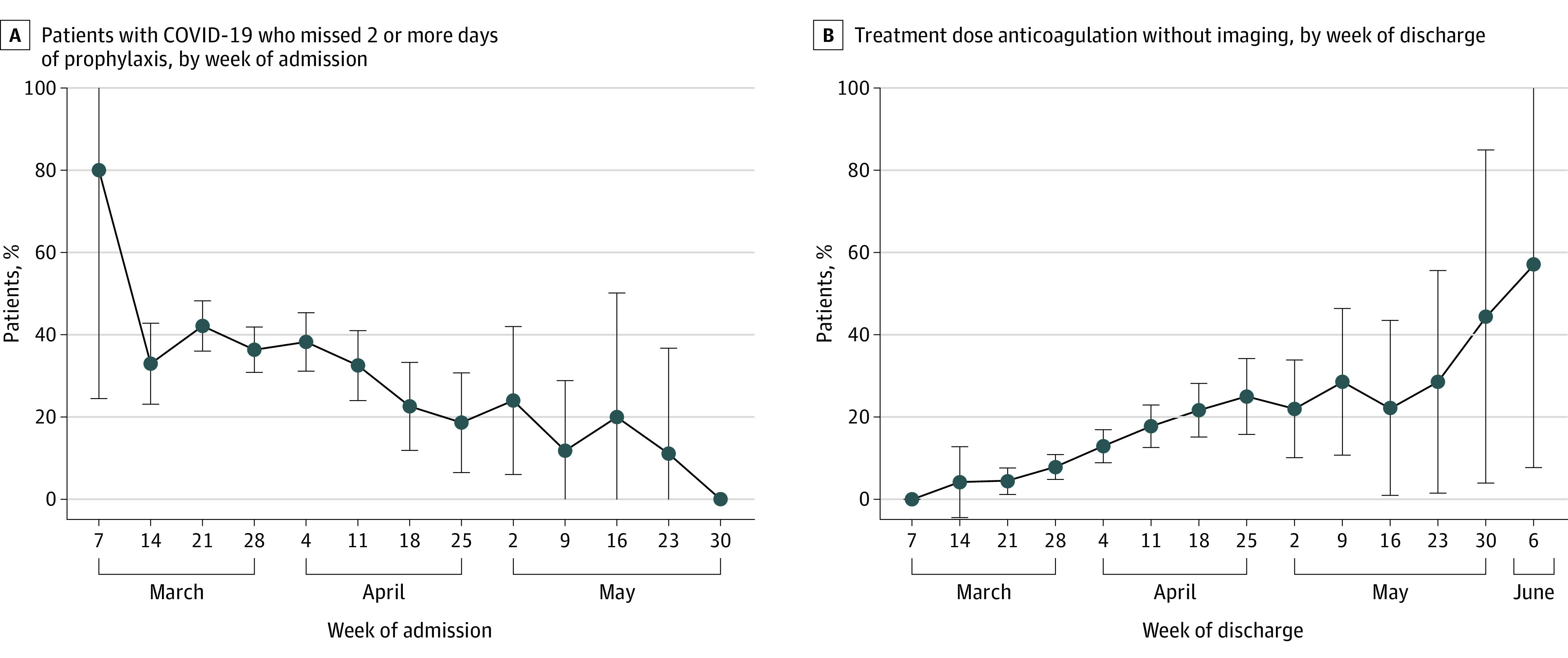
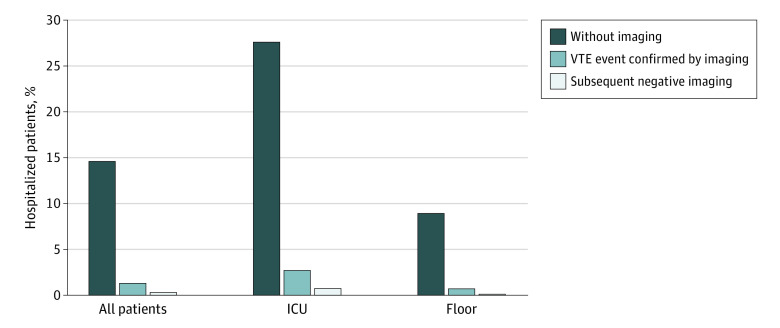
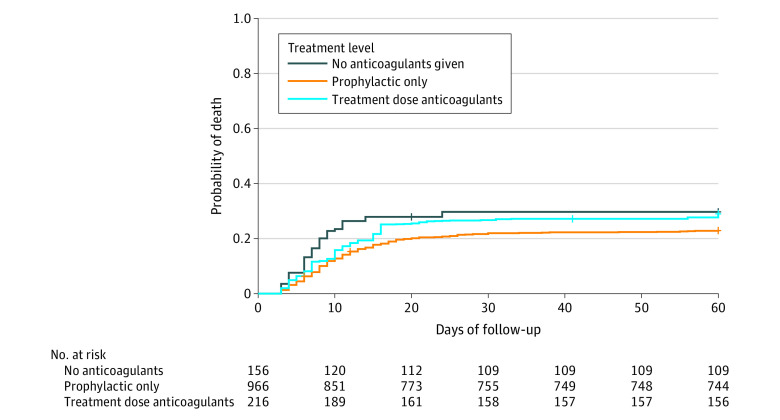
Results: Of a total 1351 patients with COVID-19 included (median [IQR] age, 64 [52-75] years; 47.7% women, 48.9% Black patients), only 18 (1.3%) had a confirmed VTE, and 219 (16.2%) received treatment-dose anticoagulation. Use of treatment-dose anticoagulation without imaging ranged from 0% to 29% across hospitals and increased over time (adjusted odds ratio [aOR], 1.46; 95% CI, 1.31-1.61 per week). Of 1127 patients who ever received anticoagulation, 392 (34.8%) missed 2 or more days of prophylaxis. Missed prophylaxis varied from 11% to 61% across hospitals and decreased markedly over time (aOR, 0.89; 95% CI, 0.82-0.97 per week). VTE nonadherence was associated with higher 60-day (adjusted hazard ratio [aHR], 1.31; 95% CI, 1.03-1.67) but not in-hospital mortality (aHR, 0.97; 95% CI, 0.91-1.03). Receiving any dose of anticoagulation (vs no anticoagulation) was associated with lower in-hospital mortality (only prophylactic dose: aHR, 0.36; 95% CI, 0.26-0.52; any treatment dose: aHR, 0.38; 95% CI, 0.25-0.58). However, only the prophylactic dose of anticoagulation remained associated with lower mortality at 60 days (prophylactic dose: aHR, 0.71; 95% CI, 0.51-0.90; treatment dose: aHR, 0.92; 95% CI, 0.63-1.35).
Conclusions and relevance: This large, multicenter cohort of patients hospitalized with COVID-19, found evidence of rapid dissemination and implementation of anticoagulation strategies, including use of treatment-dose anticoagulation. As only prophylactic-dose anticoagulation was associated with lower 60-day mortality, prophylactic dosing strategies may be optimal for patients hospitalized with COVID-19.
Conflict of interest statement
Figures
Comment in
-
Further Evidence Supporting the Use of Prophylactic Anticoagulation in Hospitalized Patients With COVID-19.JAMA Netw Open. 2021 Jun 1;4(6):e2112403. doi: 10.1001/jamanetworkopen.2021.12403. JAMA Netw Open. 2021. PMID: 34115133 No abstract available.
References
-
- Spyropoulos AC, Levy JH, Ageno W, et al. ; Subcommittee on Perioperative, Critical Care Thrombosis, Haemostasis of the Scientific, Standardization Committee of the International Society on Thrombosis and Haemostasis . Scientific and Standardization Committee communication: clinical guidance on the diagnosis, prevention, and treatment of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost. 2020;18(8):1859-1865. doi:10.1111/jth.14929 - DOI - PMC - PubMed
-
- Bikdeli B, Madhavan MV, Jimenez D, et al. ; Global COVID-19 Thrombosis Collaborative Group, Endorsed by the ISTH, NATF, ESVM, and the IUA, Supported by the ESC Working Group on Pulmonary Circulation and Right Ventricular Function . COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(23):2950-2973. doi:10.1016/j.jacc.2020.04.031 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
