

Safety Profile of the Adjuvanted Recombinant Zoster Vaccine in Immunocompromised Populations: An Overview of Six Trials
- PMID: 34115324
- PMCID: PMC8217041
- DOI: 10.1007/s40264-021-01076-w
Safety Profile of the Adjuvanted Recombinant Zoster Vaccine in Immunocompromised Populations: An Overview of Six Trials
Abstract
Introduction: The adjuvanted recombinant zoster vaccine (RZV) has demonstrated high efficacy against herpes zoster in older adults and immunocompromised populations. We present comprehensive safety data from six clinical trials in immunocompromised populations (autologous hematopoietic stem cell transplant and renal transplant recipients, patients with hematologic malignancies, patients with solid tumors, and human immunodeficiency virus-infected adults) who are at an increased risk of herpes zoster.
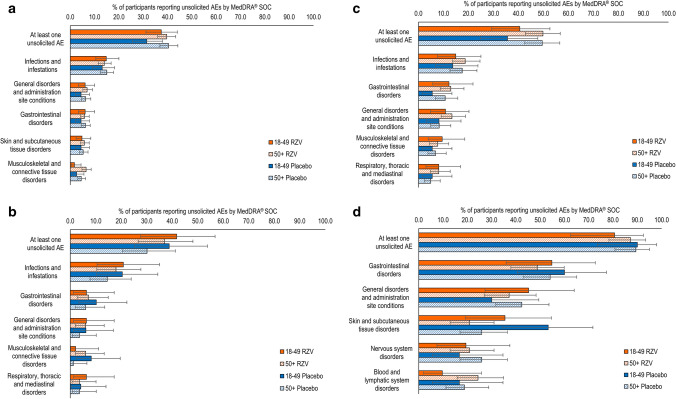
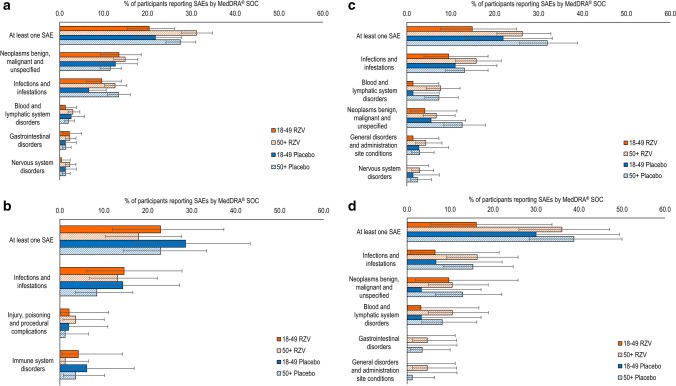
Methods: In all trials, immunocompromised adults ≥ 18 years of age were administered RZV or placebo. Safety was evaluated in the total vaccinated cohort. Solicited adverse events (AEs) were collected for 7 days and unsolicited AEs for 30 days after each dose. Serious AEs, fatal serious AEs, and potential immune-mediated diseases were collected from dose 1 until 12 months post-last dose or study end. Data were pooled for solicited AEs; unsolicited AEs, (fatal) serious AEs, and potential immune-mediated diseases were analyzed for each individual trial. All AEs were analyzed for sub-strata of adults 18-49 years of age and ≥ 50 years of age.
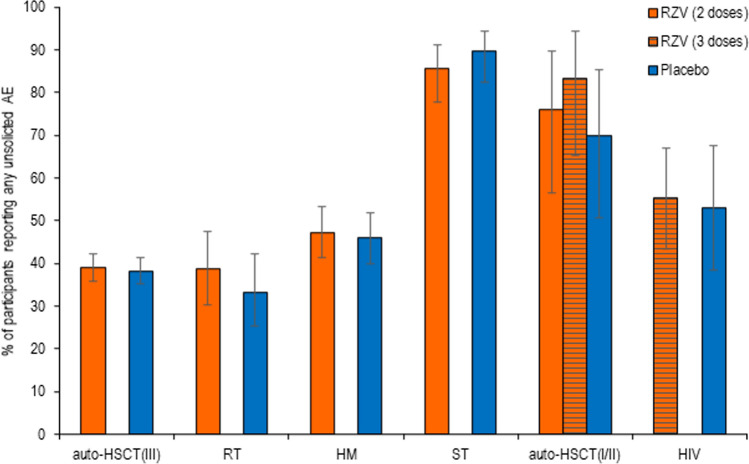
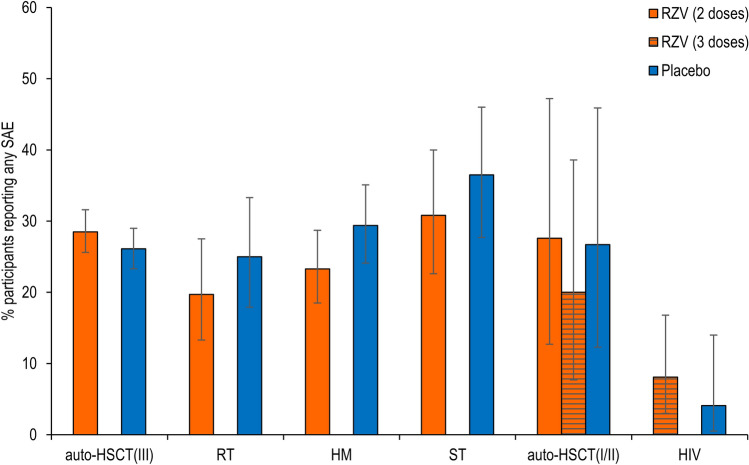
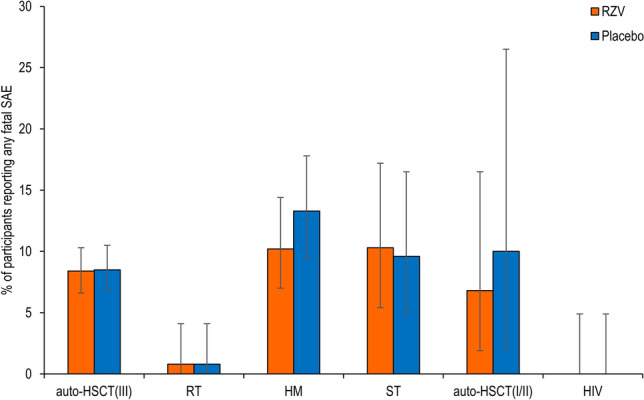
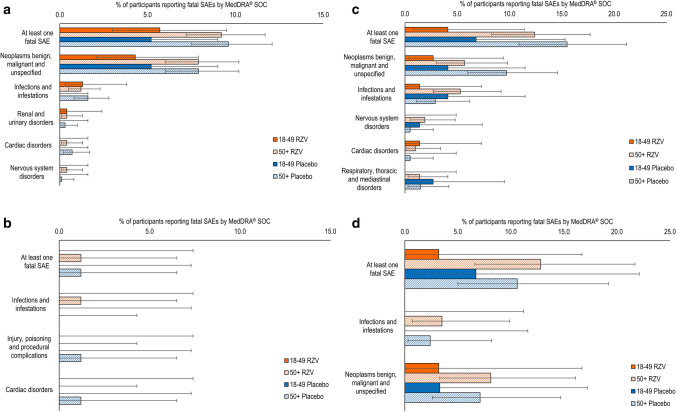
Results: In total, 1587 (RZV) and 1529 (placebo) adults were included in the pooled total vaccinated cohort. Solicited AEs were more common after RZV than placebo, were generally more common in the younger age stratum, and were mostly mild to moderate and resolved within 3 days (median duration). Unsolicited AEs and serious AEs were in line with underlying diseases and therapies. Across studies, the percentage of adults reporting one or more unsolicited AE was comparable between RZV and placebo, irrespective of age stratum. The percentage of adults reporting one or more serious AE, fatal serious AE, or potential immune-mediated diseases was generally similar for RZV and placebo, irrespective of age stratum. Overall, no safety concerns were identified.
Conclusions: Recombinant zoster vaccine has a clinically acceptable safety profile. With the previously published vaccine efficacy and immunogenicity results, these data support a favorable benefit-risk profile of RZV vaccination in immunocompromised populations who are at an increased risk of herpes zoster.
Plain language summary
Varicella zoster virus leads to chickenpox after primary infection and herpes zoster upon reactivation of the latent virus. Older adults and immunocompromised people, whose immune system is impaired because of the age-related decline in immunity and their underlying disease and/or treatment, respectively, are at an increased risk of herpes zoster and its complications. Recombinant zoster vaccine has been approved to prevent herpes zoster and its complications in adults aged ≥ 50 years in over 30 countries. In Europe, the vaccine has recently received approval to expand its use in adults aged 18 years or older who are at an increased risk of herpes zoster. We present an overview of the safety data from six clinical trials in immunocompromised patients vaccinated with recombinant zoster vaccine. We found that solicited adverse events were more common after the vaccine than placebo but that these were mild to moderate in intensity. Furthermore, the frequency of unsolicited adverse events was similar between the vaccine and placebo, and most of the reported adverse events and severe adverse events (e.g., infections or tumors) could be attributed to the pre-existent diseases and/or therapies. As such, no safety concern was identified following the review of the available clinical data. This overview, together with the published efficacy data in the prevention of herpes zoster and the vaccine immunogenicity, provides useful medical information and supports the use of the recombinant zoster vaccine in an immunocompromised population at an increased risk of herpes zoster.
Conflict of interest statement
Maribel Co-van der Mee, Pierre Beukelaers, Juan Jose Fernandez Garcia, and Fernanda Tavares-da-Silva are employed by the GSK group of companies. Marta López-Fauqued, Juan Jose Fernandez Garcia, Adriana Bastidas, Alemnew F. Dagnew, and Anne Schuind were employees of the GSK group of companies during the design, initiation, conduct of the study and/or interpretation of the data. During the conduct of the study, Pierre Beukelaers, Juan Jose Fernandez Garcia, and Fernanda Tavares-da-Silva report personal fees from the GSK group of companies. Adriana Bastidas, Pierre Beukelaers, Alemnew F. Dagnew, Anne Schuind, and Fernanda Tavares-da-Silva hold shares in the GSK group of companies.
Figures
References
-
- Tseng HF, Bruxvoort K, Ackerson B, Luo Y, Tanenbaum H, Tian Y, et al. The epidemiology of herpes zoster in immunocompetent, unvaccinated adults ≥ 50 years old: incidence, complications, hospitalization, mortality, and recurrence. J Infect Dis. 2020;222:798–806. doi: 10.1093/infdis/jiz652. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
