

Trends in Endotracheal Intubation During In-Hospital Cardiac Arrests: 2001-2018
- PMID: 34115637
- PMCID: PMC9004511
- DOI: 10.1097/CCM.0000000000005120
Trends in Endotracheal Intubation During In-Hospital Cardiac Arrests: 2001-2018
Abstract
Objectives: Airway management during in-hospital cardiac arrest represents a fundamental component of resuscitative efforts, yet little is known about temporal trends in intubation during in-hospital cardiac arrest. Our objective was to investigate changes in in-hospital cardiac arrest airway management over time and in response to national guideline updates.
Design: Observational cohort study of a prospectively collected database.
Setting: Multicenter study of hospitals participating in the "Get With The Guidelines-Resuscitation" registry from January 1, 2001, to December 31, 2018.
Subjects: Adult patients who experienced an in-hospital cardiac arrest and did not have an invasive airway in place prior to the arrest.
Interventions: The primary outcome was the rate of intra-arrest intubation from 2001 to 2018. We constructed multivariable regression models with generalized estimating equations to determine the annual adjusted odds of intubation. We also assessed the timing of intubation relative to the onset of pulselessness and other arrest measures. We used an interrupted time-series analysis to assess the association between the 2010 Advanced Cardiac Life Support guideline update and intubation rates.
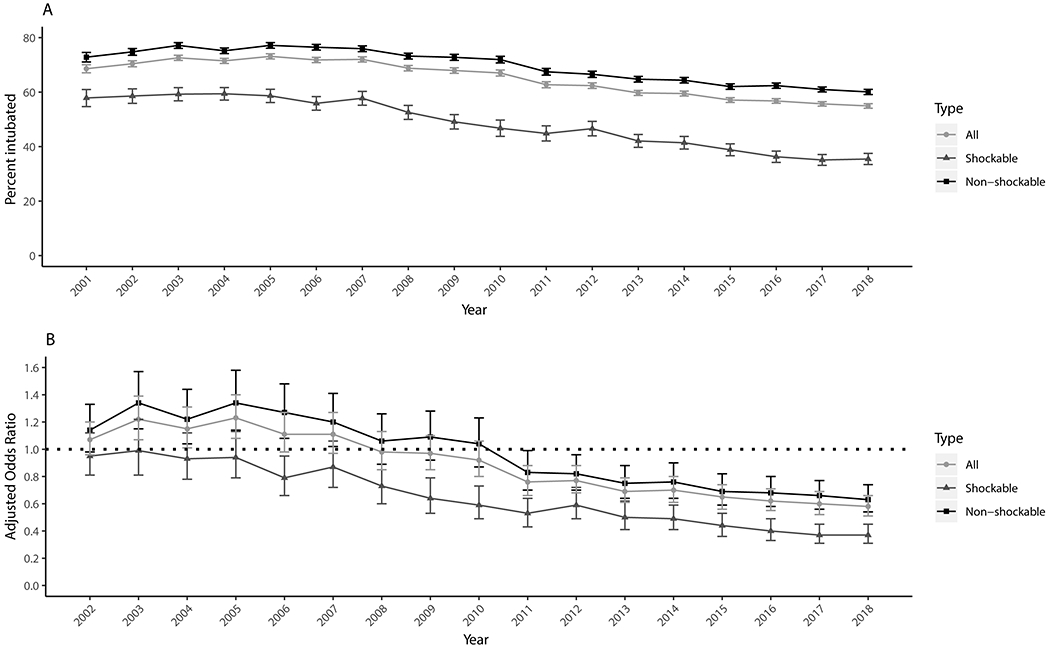
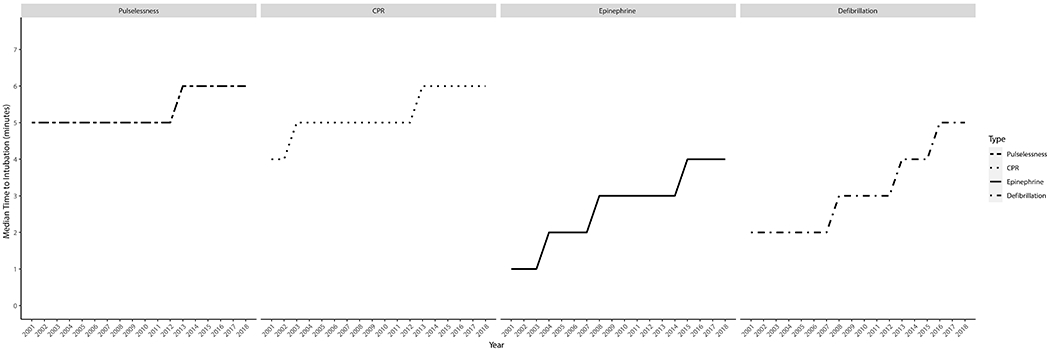
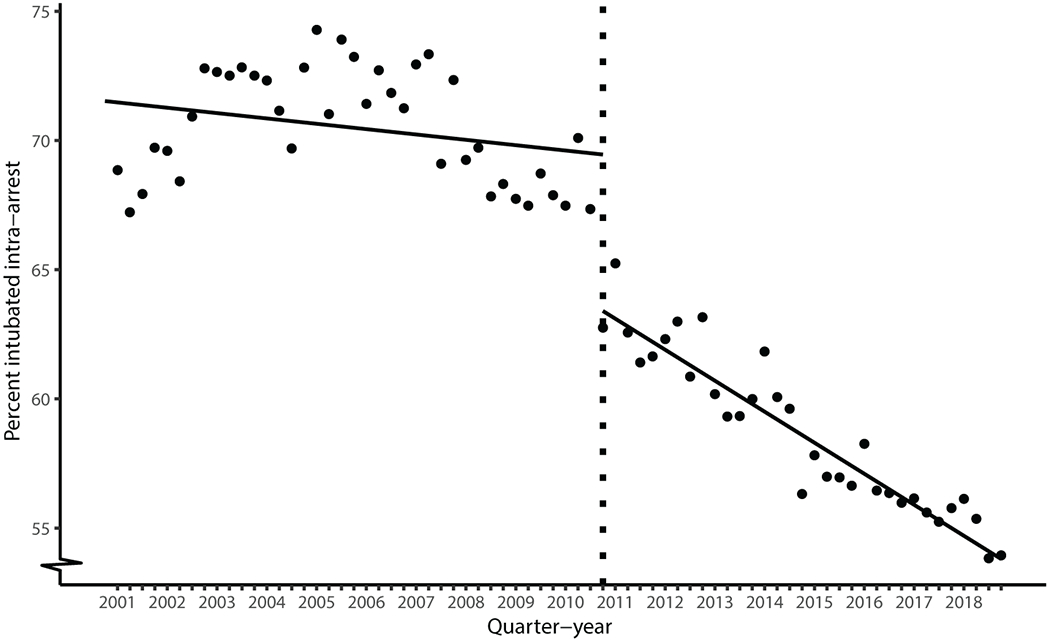
Measurements and main results: One thousand sixty-six eight hundred patients from 797 hospitals were included. From 2001 to 2018, the percentage of patients intubated during an arrest decreased from 69% to 55% for all rhythms, 73% to 60% for nonshockable rhythms, and 58% to 36% for shockable rhythms (p < 0.001 for trend for all 3 groups). The median time from onset of pulselessness to intubation increased from 5 minutes in 2001 (interquartile range, 2-8 min) to 6 minutes in 2018 (interquartile range, 4-10 min) (p < 0.001 for trend). Following the 2010 guideline update, there was a downward step change and a steeper decrease over time in the rate of intubation as compared to the preintervention period (p < 0.001).
Conclusions: Endotracheal intubation rates during in-hospital cardiac arrest have decreased significantly over time, with a more substantial decline following the updated 2010 guideline that prioritized chest compressions over airway management.
Copyright © 2021 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved.
Conflict of interest statement
Dr. Buhr’s institution received funding from the National Institutes of Health (NIH) National Center for Advancing Translational Sciences (NCATS); he received funding from the NIH/NCATS (KL2TR001882), the National Heart, Lung, and Blood Institute (NHLBI), and the University of California Office of the President; he received personal consulting fees from Mylan/Theravance Biopharma and GlaxoSmithKline; he disclosed he is employed part-time by the Veterans Health Administration; he received support for article research from the NIH. This work does not necessarily represent the views and opinions of the Department of Veterans Affairs. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Field JM, Hazinski MF, Sayre MR, Chameides L, Schexnayder SM, Hemphill R, et al. Part 1: executive summary: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010; - PubMed
-
- Neumar RW, Otto CW, Link MS, Kronick SL, Shuster M, Callaway CW, et al. Part 8: Adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010. - PubMed
-
- Link MS, Berkow LC, Kudenchuk PJ, Halperin HR, Hess EP, Moitra VK, et al. Part 7: Adult advanced cardiovascular life support: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015; - PubMed
