

Pneumocephalus with meningitis secondary to an old traumatic anterior cranial fossa defect
- PMID: 34116999
- PMCID: PMC8201975
- DOI: 10.1136/bcr-2021-242855
Pneumocephalus with meningitis secondary to an old traumatic anterior cranial fossa defect
Abstract
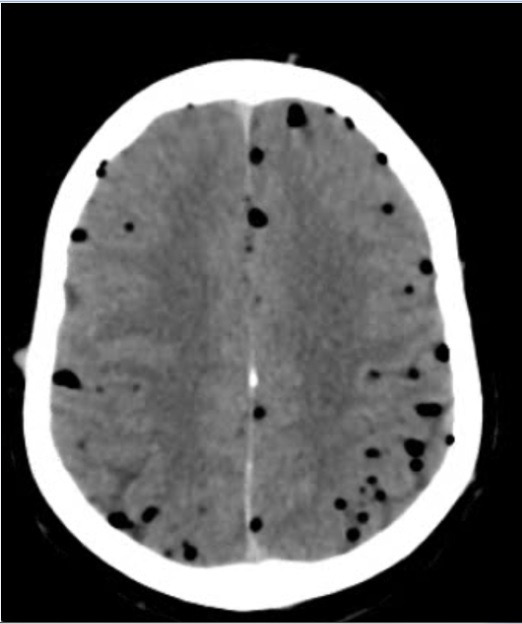
We report a case of a 30-year-old man who presented with altered mental status, fever, headache and vomiting for 3 days. An initial CT scan of the brain revealed the presence of pneumocephalus with a bony defect in the anterior cranial fossa. The pneumocephalus was not explained initially and the patient was re-examined for any signs of trauma to the face, and a review of the history revealed a series of three traumatic events months prior to this illness. Further laboratory studies revealed Streptococcus pneumoniae in the blood and bacterial meningitis. He was treated with antibiotics and was later taken up for endoscopic repair of the skull base defect. This case highlights the importance of recognising post-traumatic pneumocephalus with superimposed meningitis and sepsis months after a traumatic event to the skull base.
Keywords: emergency medicine; infection (neurology); meningitis; otolaryngology / ENT; trauma.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous