

Overweight and Obesity and Progression of ADPKD
- PMID: 34117082
- PMCID: PMC8216617
- DOI: 10.2215/CJN.16871020
Overweight and Obesity and Progression of ADPKD
Abstract
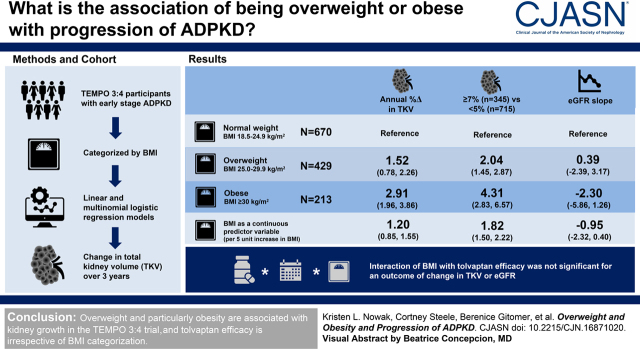
Background and objectives: On the basis of earlier observations, we evaluated the association between overweight and obesity and rapid progression of autosomal dominant polycystic kidney disease in participants in the Tolvaptan Efficacy and Safety in Management of Autosomal Dominant Polycystic Kidney Disease and Its Outcomes (TEMPO) 3:4 trial. More importantly, we also determined whether efficacy of tolvaptan was attenuated in individuals with baseline overweight or obesity.
Design, setting, participants, & measurements: A total of 1312 study participants with relatively early-stage autosomal dominant polycystic kidney disease (mean eGFR 78±22 ml/min per 1.73 m2) who were at high risk of rapid progression were categorized by body mass index (BMI; calculated using nonkidney weight) as normal weight (18.5-24.9 kg/m2; n=670), overweight (25.0-29.9 kg/m2; n=429), or obese (≥30 kg/m2; n=213). Linear and multinomial logistic regression models were used to determine the association of baseline overweight and obesity with change in total kidney volume (TKV) over the 3-year study period.
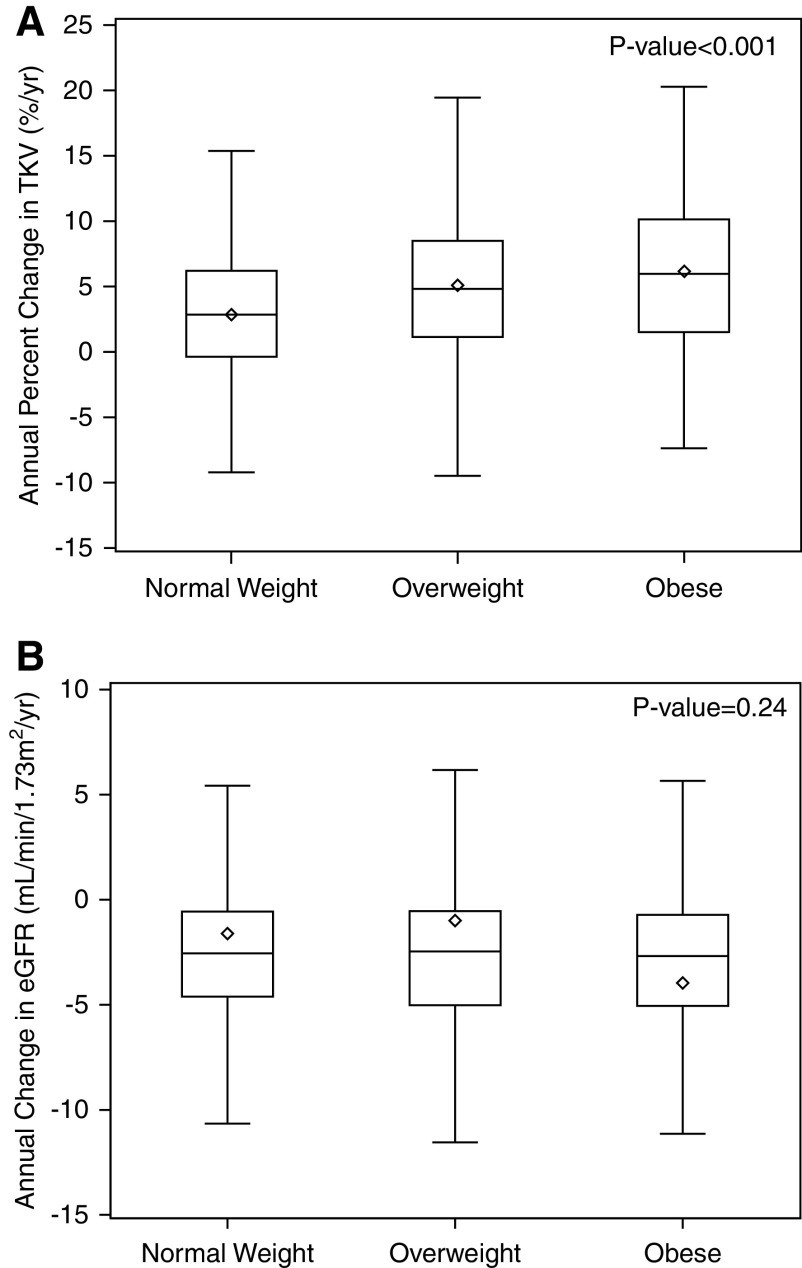
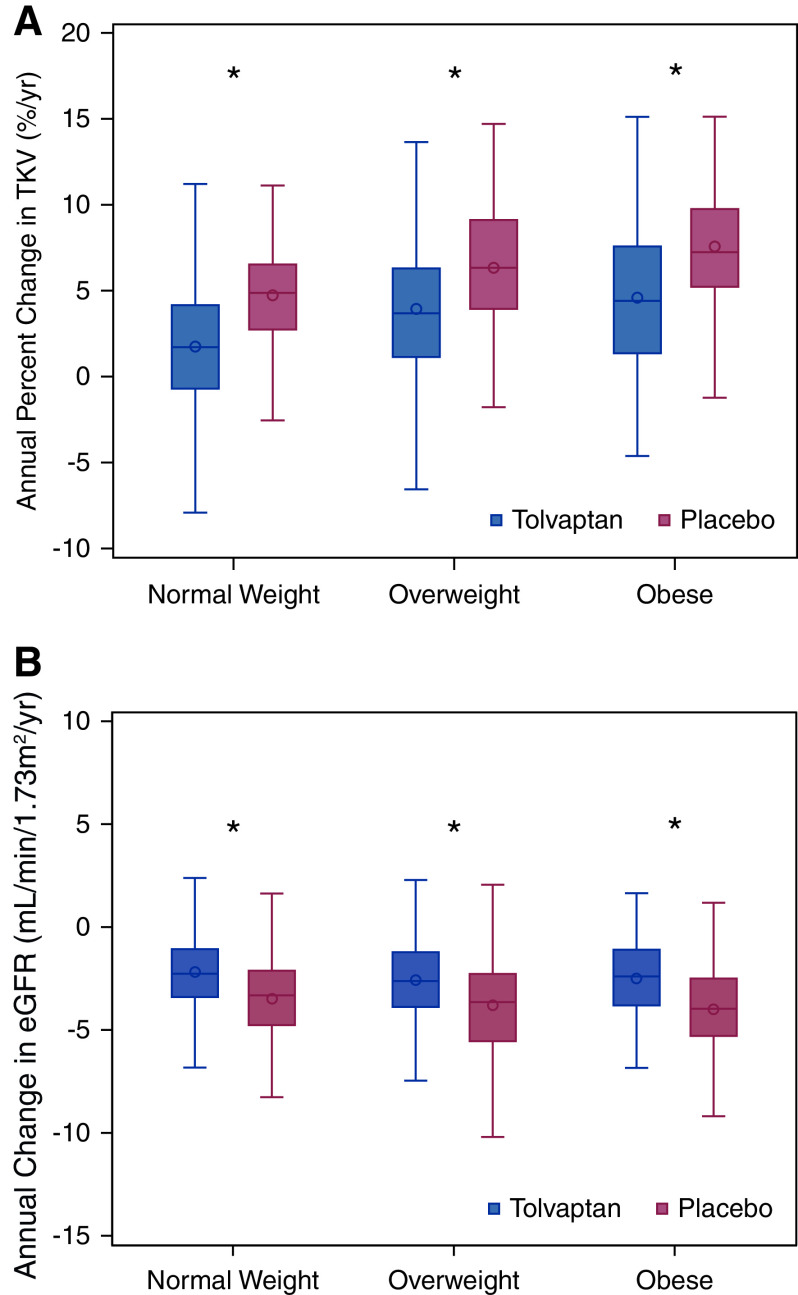
Results: In fully adjusted models, higher BMI was associated with greater annual percent change in TKV (difference of 1.20 [95% confidence interval (95% CI), 0.85 to 1.55] per five-unit higher BMI). Overweight and obesity were associated with higher odds of annual percent change in TKV of ≥7% versus <5% (overweight: odds ratio, 2.04 [95% CI, 1.45 to 2.87]; obese: odds ratio, 4.31 [95% CI, 2.83 to 6.57] versus normal weight). eGFR decline did not differ according to BMI (fully adjusted difference in decline of -0.95 [95% CI, -2.32 to 0.40] ml/min per 1.73 m2 per year per five-unit higher BMI). The three-way interaction (treatment×time×BMI group) was not statistically significant in linear mixed models with an outcome of TKV (log-transformed estimated coefficient comparing the treatment effect for overweight versus normal weight: 0.56% [95% CI, -0.70% to 1.84%] per year; P=0.38; obese versus normal weight: 0.07% [95% CI, -1.47% to 1.63%] per year; P=0.93) or eGFR (estimated coefficient comparing overweight versus normal weight: -0.07 [95% CI, -0.95 to 0.82] ml/min per 1.73 m2 per year; P=0.88; obese versus normal weight: 0.22 [95% CI, -0.93 to 1.36] ml/min per 1.73 m2 per year; P=0.71).
Conclusions: Overweight and particularly obesity are strongly and independently associated with kidney growth, but not eGFR slope, in the TEMPO 3:4 trial, and tolvaptan efficacy is irrespective of BMI categorization.
Clinical trial registry name and registration number: Tolvaptan Efficacy and Safety in Management of Autosomal Dominant Polycystic Kidney Disease and Its Outcomes (TEMPO) 3:4, NCT00428948.
Keywords: ADPKD; disease progression; epidemiology and outcomes; obesity; overweight; polycystic kidney disease.
Copyright © 2021 by the American Society of Nephrology.
Figures
Comment in
-
To Add Weight to Overweight.Clin J Am Soc Nephrol. 2021 Jun;16(6):850-852. doi: 10.2215/CJN.04150321. Clin J Am Soc Nephrol. 2021. PMID: 34117079 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
