

Impact of Adjuvant Medical Therapies on Surgical Outcomes in Idiopathic Subglottic Stenosis
- PMID: 34117778
- PMCID: PMC8762605
- DOI: 10.1002/lary.29675
Impact of Adjuvant Medical Therapies on Surgical Outcomes in Idiopathic Subglottic Stenosis
Abstract
Objectives/hypothesis: Adjuvant medications including proton pump inhibitors (PPI), antibiotics (trimethoprim/sulfamethoxazole [TMP-SMX]), and inhaled corticosteroids (ICS) may be prescribed for patients with idiopathic subglottic stenosis (iSGS). We describe medication use with endoscopic dilation (ED) or endoscopic resection with medical treatment (ERMT) and evaluate impact on outcomes.
Study design: International, prospective, 3-year multicenter cohort study of 810 patients with untreated, newly diagnosed, or previously treated iSGS.
Methods: Post hoc secondary analysis of prospectively collected North American Airway Collaborative data on outcomes linked with adjuvant medication utilization. Primary outcome was time to recurrent operation, evaluated using Kaplan-Meier curves and Cox regression analysis. Secondary outcomes of change in peak expiratory flow (PEF) and clinical chronic obstructive pulmonary disease questionnaire (CCQ) score over 12 months were compared.
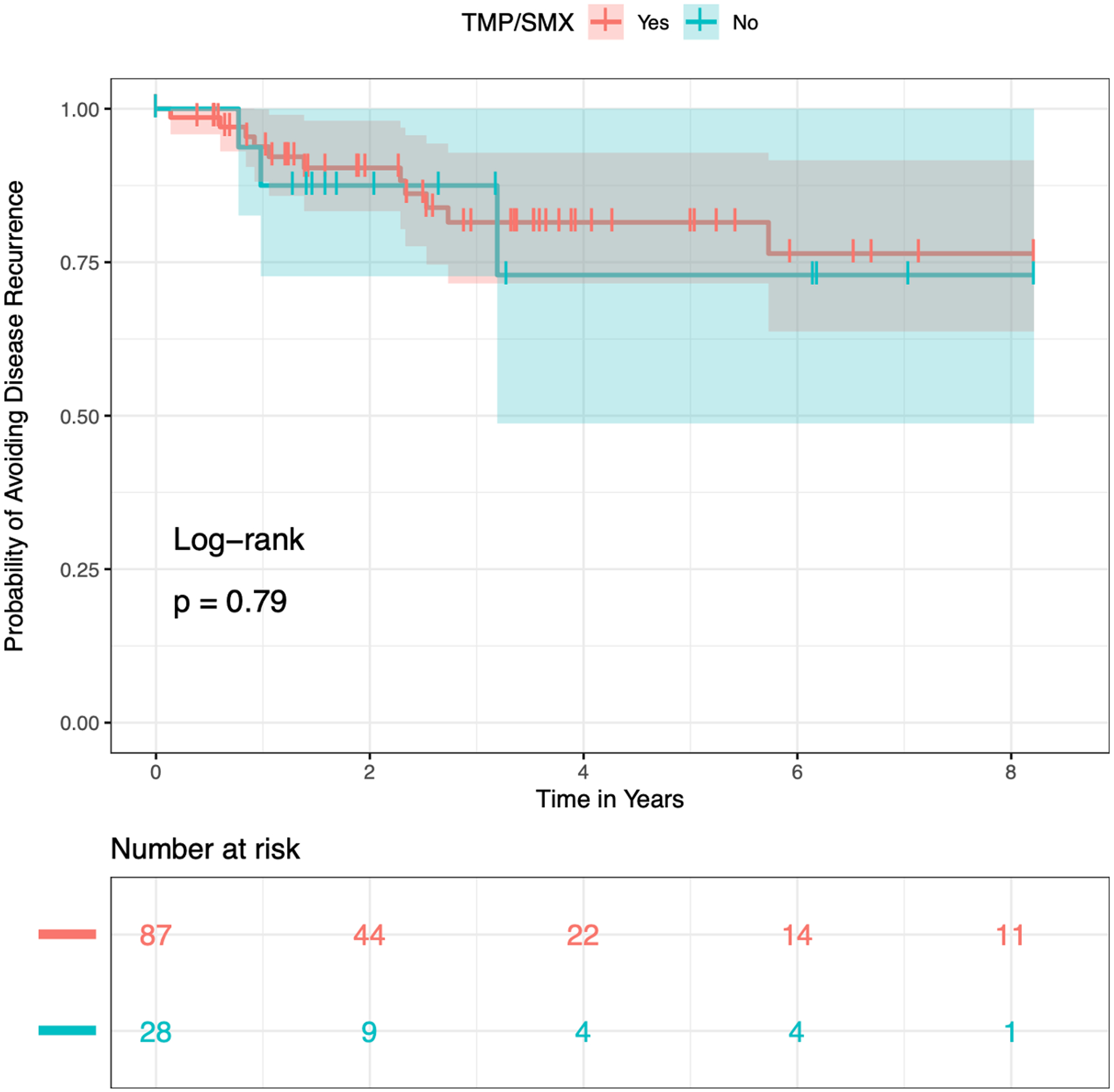
Results: Sixty-one of 129 patients undergoing ED received PPI (47%), and 10/143 patients undergoing ED received ICS (7%). TMP-SMX was used by 87/115 patients (76%) undergoing EMRT. PPI use in the ED group did not affect time to recurrence (hazard ratio [HR] = 1.00, 95% confidence interval [CI]: 0.53-1.88; P = .99) or 12-month change in PEF (L/min) (median [interquartile range], 12.0 [10.7-12.2] vs. 8.7 [-5.1 to 24.9]; P = .59), but was associated with 12-month change in CCQ (-0.05 [-0.97 to 0.75] vs. -0.50 [-1.60 to 0.20]; P = .04). ICS did not affect outcome measures. TMP-SMX use in ERMT did not affect time to recurrence (HR = 0.842, 95% CI: 0.2345-3.023; P = .79), PEF at 12 months (75 [68-89] vs. 81 [68-89]; P = .92), or 12-month change in CCQ (0.20 [-1.05 to 0.47] vs. -0.30 [-1.00 to 0.10]; P = .45).
Conclusion: There is no standard practice for prescribing adjuvant medications. These data do not support that adjuvant medications prolong time to recurrence or increase PEF. Patients with iSGS and gastroesophageal reflux disease may experience some symptom benefit with PPI.
Level of evidence: 3 Laryngoscope, 131:E2880-E2886, 2021.
Keywords: Idiopathic subglottic stenosis; adjuvant medical treatment; endoscopic dilation; endoscopic resection with medical therapy; inhaled corticosteroid; proton pump inhibitor; trimethoprim-sulfamethoxazole.
© 2021 The American Laryngological, Rhinological and Otological Society, Inc..
Conflict of interest statement
Figures


References
-
- Mark EJ, Meng F, Kradin RL, Mathisen DJ, Matsubara O. Idiopathic tracheal stenosis: A clinicopathologic study of 63 cases and comparison of the pathology with chondromalacia. Am J Surg Pathol 2008; 32:1138–43. - PubMed
-
- Maldonado F, Loiselle A, DePew ZS, et al. Idiopathic subglottic stenosis: An evolving therapeutic algorithm. Laryngoscope 2014; 124:498–503. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
