

Emergency endoscopic surgery for pituitary apoplexy presenting as cerebral infarction in a limited resources condition: A case report
- PMID: 34118525
- PMCID: PMC8193137
- DOI: 10.1016/j.ijscr.2021.106015
Emergency endoscopic surgery for pituitary apoplexy presenting as cerebral infarction in a limited resources condition: A case report
Abstract
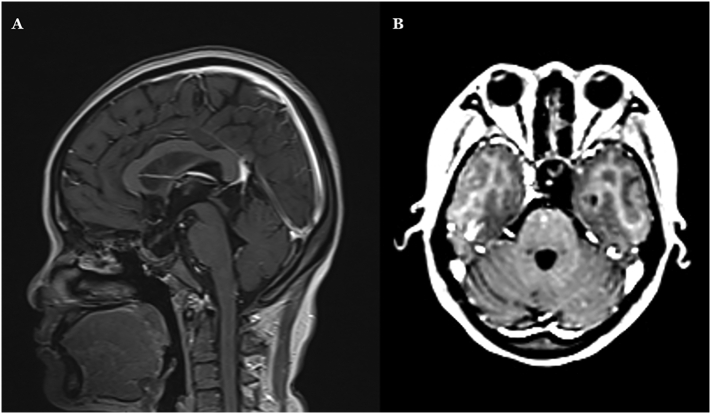
Introduction and importance: Pituitary apoplexy is defined as a sudden onset of neurologic deficit due to infarction or hemorrhage of the pituitary tumor. We report a case of emergency endoscopic surgery for pituitary apoplexy presenting as cerebral infarction due to ICA compression in a limited resources condition.
Case presentation: A 38-year-old female presented with acute onset of severe headache, decreased level of consciousness, decreased visual acuity bilaterally, aphasia, and right hemiparesis. Computed tomography angiography showed a hyperdense sellar mass with stenosis of the left ICA. The patient underwent emergent endoscopic transsphenoidal surgery for sellar decompression.
Clinical discussion: The epidermiology, presentation and diagnosis and strategy of treatments as well as their outcomes were discussed.
Conclusion: Pituitary apoplexy should be taken into consideration in a patient with increasing headache and neuro-ophthalmic symptoms. Pituitary apoplexy presenting as cerebral infarction is rare. The aim of surgery in emergency setting was sellar decompression. Endoscopic transsphenoidal surgery was an effective treatment.
Keywords: Cerebral infarction; Endoscopic transsphenoidal surgery; Pituitary adenoma; Pituitary apoplexy.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
The authors declared no conflict of interest.
Figures






References
-
- A D., Ronquillo Yasmyne. Snellen Chart. Text. 2020. https://www.ncbi.nlm.nih.gov/books/NBK558961/ 2020/06/10.
LinkOut - more resources
Full Text Sources
Miscellaneous
