

Effects of levosimendan on renal blood flow and glomerular filtration in patients with acute kidney injury after cardiac surgery: a double blind, randomized placebo-controlled study
- PMID: 34118980
- PMCID: PMC8199833
- DOI: 10.1186/s13054-021-03628-z
Effects of levosimendan on renal blood flow and glomerular filtration in patients with acute kidney injury after cardiac surgery: a double blind, randomized placebo-controlled study
Abstract
Background: Acute kidney injury (AKI) is a common and serious complication after cardiac surgery, and current strategies aimed at treating AKI have proven ineffective. Levosimendan, an inodilatating agent, has been shown to increase renal blood flow and glomerular filtration rate in uncomplicated postoperative patients and in patients with the cardiorenal syndrome. We hypothesized that levosimendan through its specific effects on renal vasculature, a preferential vasodilating effect on preglomerular resistance vessels, could improve renal function in AKI-patients with who did not have clinical indication for inotropic support.
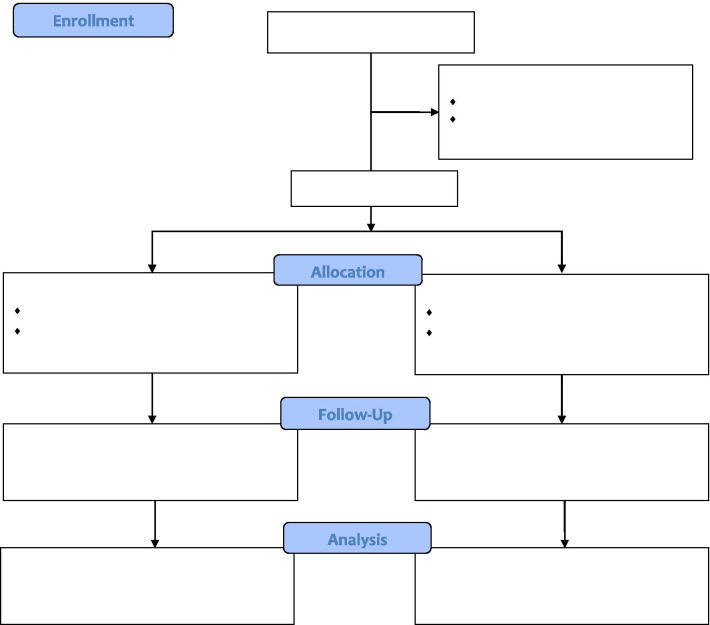
Methods: In this single-center, double-blind, randomized controlled study, adult patients with postoperative AKI within 2 days after cardiac surgery, who were hemodynamically stable with a central venous oxygen saturation (ScvO2) ≥ 60% without inotropic support were eligible for inclusion. After randomization, study drug infusions, levosimendan (n = 16) or placebo (n = 13) were given for 5 h. A bolus infusion of levosimendan (12 µg/kg), were given for 30 min followed by 0.1 µg/kg/min for 5 h. Renal blood flow and glomerular filtration rate were measured using infusion clearance of para-aminohippuric acid and a filtration marker, respectively. As a safety issue, norepinephrine was administered to maintain mean arterial pressure between 70-80 mmHg. Intra-group differences were tested by Mann-Whitney U-tests, and a linear mixed model was used to test time and group interaction.
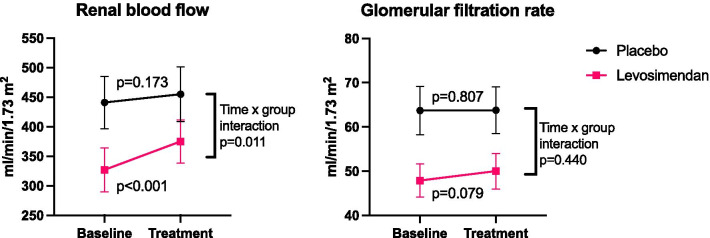
Results: Twenty-nine patients completed the study. At inclusion, the mean serum creatinine was higher in the patients randomized to levosimendan (148 ± 29 vs 127 ± 22 µmol/L, p = 0.030), and the estimated GFR was lower (46 ± 12 vs 57 ± 11 ml/min/1.73 m2, p = 0.025). Levosimendan induced a significantly (p = 0.011) more pronounced increase in renal blood flow (15%) compared placebo (3%) and a more pronounced decrease in renal vascular resistance (- 18% vs. - 4%, respectively, p = 0.043). There was a trend for a minor increase in glomerular filtration rate with levosimendan (4.5%, p = 0.079), which did differ significantly from the placebo group (p = 0.440). The mean norepinephrine dose was increased by 82% in the levosimedan group and decreased by 29% in the placebo group (p = 0.012).
Conclusions: In hemodynamically stable patients with AKI after cardiac surgery, levosimendan increases renal blood flow through renal vasodilatation. Trial registration NCT02531724, prospectly registered on 08/20/2015. https://clinicaltrials.gov/ct2/show/NCT02531724?cond=AKI&cntry=SE&age=1&draw=2&rank=1.
Conflict of interest statement
Lukas Lannemyr and Sven-Erik Ricksten have received speaker honorarium from Orion Pharma.
Figures
Similar articles
-
Effects of levosimendan on glomerular filtration rate, renal blood flow, and renal oxygenation after cardiac surgery with cardiopulmonary bypass: a randomized placebo-controlled study.Crit Care Med. 2013 Oct;41(10):2328-35. doi: 10.1097/CCM.0b013e31828e946a. Crit Care Med. 2013. PMID: 23921271 Clinical Trial.
-
Effect of Levosimendan on Renal Outcome in Cardiac Surgery Patients With Chronic Kidney Disease and Perioperative Cardiovascular Dysfunction: A Substudy of a Multicenter Randomized Trial.J Cardiothorac Vasc Anesth. 2018 Oct;32(5):2152-2159. doi: 10.1053/j.jvca.2018.02.039. Epub 2018 Feb 26. J Cardiothorac Vasc Anesth. 2018. PMID: 29580796 Clinical Trial.
-
Differential Effects of Levosimendan and Dobutamine on Glomerular Filtration Rate in Patients With Heart Failure and Renal Impairment:A Randomized Double-Blind Controlled Trial.J Am Heart Assoc. 2018 Aug 21;7(16):e008455. doi: 10.1161/JAHA.117.008455. J Am Heart Assoc. 2018. PMID: 30369310 Free PMC article. Clinical Trial.
-
Levosimendan Reduces Mortality and Low Cardiac Output Syndrome in Cardiac Surgery.Thorac Cardiovasc Surg. 2020 Aug;68(5):401-409. doi: 10.1055/s-0039-3400496. Epub 2019 Nov 26. Thorac Cardiovasc Surg. 2020. PMID: 31770777
-
Levosimendan: a new inodilatory drug for the treatment of decompensated heart failure.Curr Pharm Des. 2005;11(4):435-55. doi: 10.2174/1381612053382043. Curr Pharm Des. 2005. PMID: 15725064 Review.
Cited by
-
Proteomics-based screening of AKR1B1 as a therapeutic target and validation study for sepsis-associated acute kidney injury.PeerJ. 2024 Jan 2;12:e16709. doi: 10.7717/peerj.16709. eCollection 2024. PeerJ. 2024. PMID: 38188141 Free PMC article.
-
Sepsis-associated acute kidney injury: consensus report of the 28th Acute Disease Quality Initiative workgroup.Nat Rev Nephrol. 2023 Jun;19(6):401-417. doi: 10.1038/s41581-023-00683-3. Epub 2023 Feb 23. Nat Rev Nephrol. 2023. PMID: 36823168 Review.
-
Levosimendan in acute heart failure with severely reduced kidney function, a propensity score matched registry study.Front Cardiovasc Med. 2022 Oct 20;9:1027727. doi: 10.3389/fcvm.2022.1027727. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36337866 Free PMC article.
-
Advances of perioperative acute kidney injury in elderly patients undergoing non-cardiac surgery.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023 May 28;48(5):760-770. doi: 10.11817/j.issn.1672-7347.2023.220629. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 37539579 Free PMC article. Chinese, English.
-
Levosimendan in intensive care and emergency medicine: literature update and expert recommendations for optimal efficacy and safety.J Anesth Analg Crit Care. 2022 Jan 24;2(1):4. doi: 10.1186/s44158-021-00030-7. J Anesth Analg Crit Care. 2022. PMID: 37386589 Free PMC article. Review.
References
-
- Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, Bauer P, Hiesmayr M. Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol. 2004;15(6):1597–1605. doi: 10.1097/01.ASN.0000130340.93930.DD. - DOI - PubMed
-
- Nadim MK, Forni LG, Bihorac A, Hobson C, Koyner JL, Shaw A, Arnaoutakis GJ, Ding X, Engelman DT, Gasparovic H et al: Cardiac and Vascular Surgery-Associated Acute Kidney Injury: The 20th International Consensus Conference of the ADQI (Acute Disease Quality Initiative) Group. J Am Heart Assoc. 2018, 7(11). - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
