

SCORE2-OP risk prediction algorithms: estimating incident cardiovascular event risk in older persons in four geographical risk regions
- PMID: 34120185
- PMCID: PMC8248997
- DOI: 10.1093/eurheartj/ehab312
SCORE2-OP risk prediction algorithms: estimating incident cardiovascular event risk in older persons in four geographical risk regions
Abstract
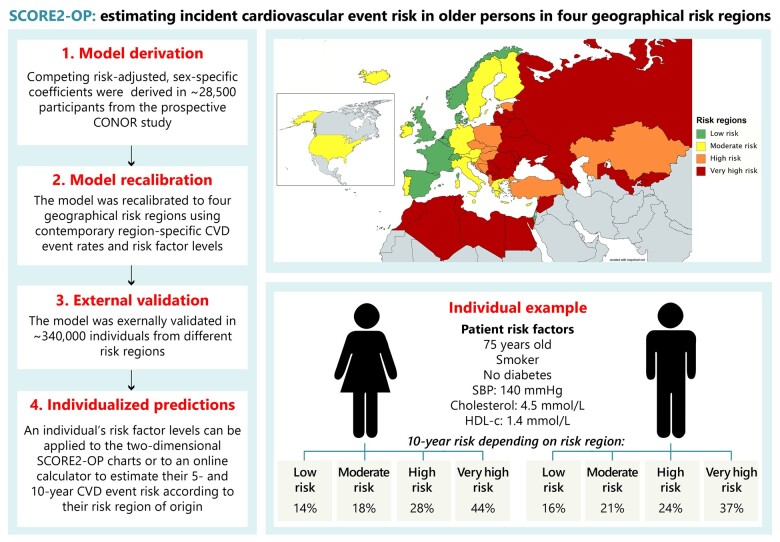
Aims: The aim of this study was to derive and validate the SCORE2-Older Persons (SCORE2-OP) risk model to estimate 5- and 10-year risk of cardiovascular disease (CVD) in individuals aged over 70 years in four geographical risk regions.
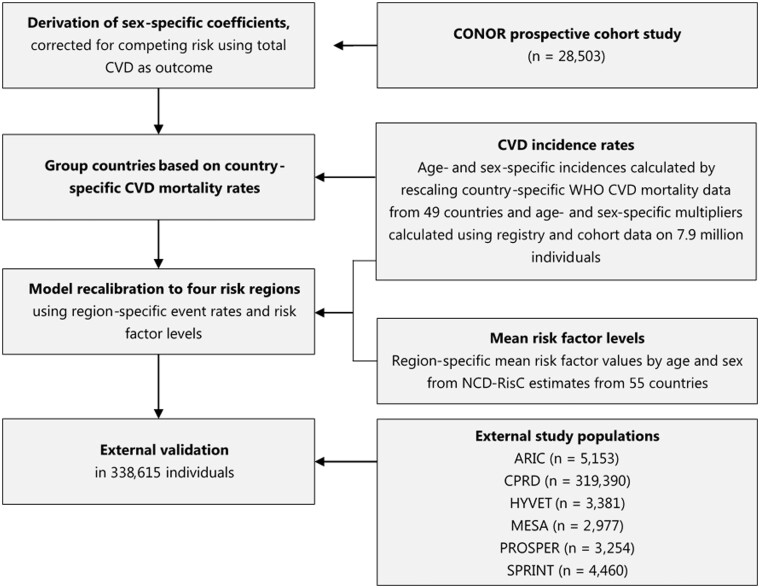
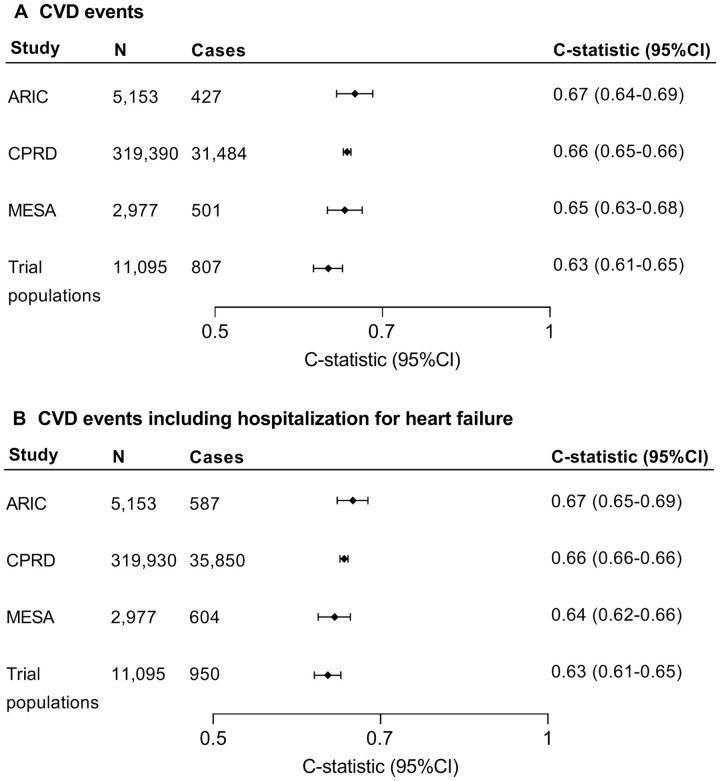
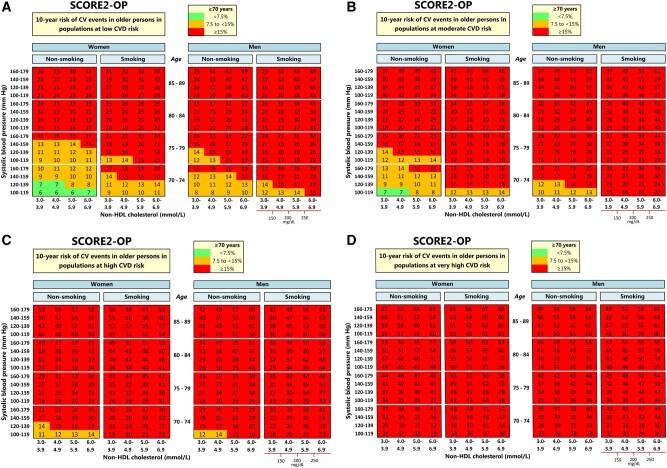
Methods and results: Sex-specific competing risk-adjusted models for estimating CVD risk (CVD mortality, myocardial infarction, or stroke) were derived in individuals aged over 65 without pre-existing atherosclerotic CVD from the Cohort of Norway (28 503 individuals, 10 089 CVD events). Models included age, smoking status, diabetes, systolic blood pressure, and total- and high-density lipoprotein cholesterol. Four geographical risk regions were defined based on country-specific CVD mortality rates. Models were recalibrated to each region using region-specific estimated CVD incidence rates and risk factor distributions. For external validation, we analysed data from 6 additional study populations {338 615 individuals, 33 219 CVD validation cohorts, C-indices ranged between 0.63 [95% confidence interval (CI) 0.61-0.65] and 0.67 (0.64-0.69)}. Regional calibration of expected-vs.-observed risks was satisfactory. For given risk factor profiles, there was substantial variation across the four risk regions in the estimated 10-year CVD event risk.
Conclusions: The competing risk-adjusted SCORE2-OP model was derived, recalibrated, and externally validated to estimate 5- and 10-year CVD risk in older adults (aged 70 years or older) in four geographical risk regions. These models can be used for communicating the risk of CVD and potential benefit from risk factor treatment and may facilitate shared decision-making between clinicians and patients in CVD risk management in older persons.
Keywords: 10-Year CVD risk; Cardiovascular disease; Older persons; Primary prevention; Risk assessment; Risk prediction.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Redefining cardiovascular risk prediction: is the crystal ball clearer now?Eur Heart J. 2021 Jul 1;42(25):2468-2471. doi: 10.1093/eurheartj/ehab310. Eur Heart J. 2021. PMID: 34120165 No abstract available.
References
-
- Stam-Slob MC, Visseren FLJ, Jukema J, Graaf Y. V D, Poulter NR, Gupta A, Sattar N, Macfarlane PW, Kearney PM, Craen A. D, Trompet S. Personalized absolute benefit of statin treatment for primary or secondary prevention of vascular disease in individual elderly patients. Clin Res Cardiol 2017;106:58–68. - PMC - PubMed
-
- Wolbers M, Koller MT, Witteman JCM, Steyerberg EW. Prognostic models with competing risks: methods and application to coronary risk prediction. Epidemiology 2009;20:555–561. - PubMed
-
- Hohl CM, Dankoff J, Colacone A, Afilalo M. Polypharmacy, adverse drug-related events, and potential adverse drug interactions in elderly patients presenting to an emergency department. Ann Emerg Med 2001;38:666–671. - PubMed
Publication types
MeSH terms
Grants and funding
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- 75N92020D00001/NH/NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- NS/NINDS NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- AG/NIA NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- RG/13/13/30194/BHF_/British Heart Foundation/United Kingdom
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- RG/18/13/33946/BHF_/British Heart Foundation/United Kingdom
- HHSN268201700001I/NH/NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- UL1-TR-000040/NH/NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- CH/12/2/29428/BHF_/British Heart Foundation/United Kingdom
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
