

doi: 10.1161/HYPERTENSIONAHA.121.17436.
Epub 2021 Jun 14.
Renal Injuries in Primary Aldosteronism: Quantitative Histopathological Analysis of 19 Patients With Primary Adosteronism
Affiliations
- PMID: 34120452
- PMCID: PMC8597934
- DOI: 10.1161/HYPERTENSIONAHA.121.17436
Item in Clipboard
Renal Injuries in Primary Aldosteronism: Quantitative Histopathological Analysis of 19 Patients With Primary Adosteronism
Hypertension.
2021 Aug.
Abstract
[Figure: see text].
Keywords: 11βHSD; aldosterone; histopathology; hypertension; mineralocorticoid receptor; renin.
Figures
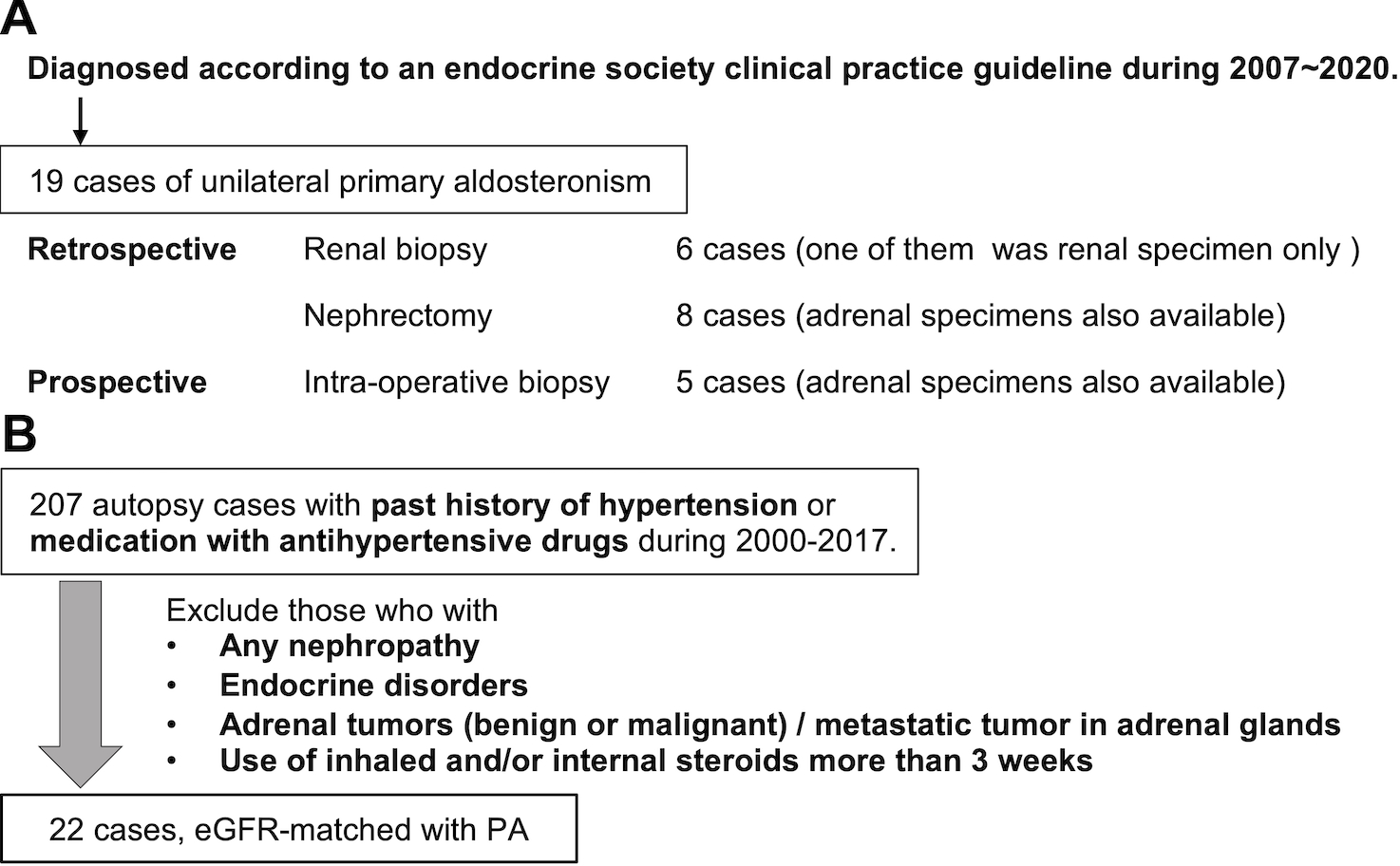
A. Selection of PA cases. We studied 19 APA cases in this study. Fourteen of renal specimens were retrospectively and 5 prospectively obtained. Retrospective cohort contained 6 renal biopsy and 8 nephrectomy cases. Prospective cohort underwent intraoperative renal biopsy. B. Selection of EH cases. We collected 207 EH cases with past history of hypertension or use of antihypertensive agents from autopsy cases performed in Tohoku University Hospital from 2000 to 2017. We excluded those who had any nephropathies or endocrine disorders, had adrenal tumor both benign and malignant, and were given inhaled or/and medication of steroids more than 3 weeks. After that, 22 cases with matched eGFR with PA were retrieved.
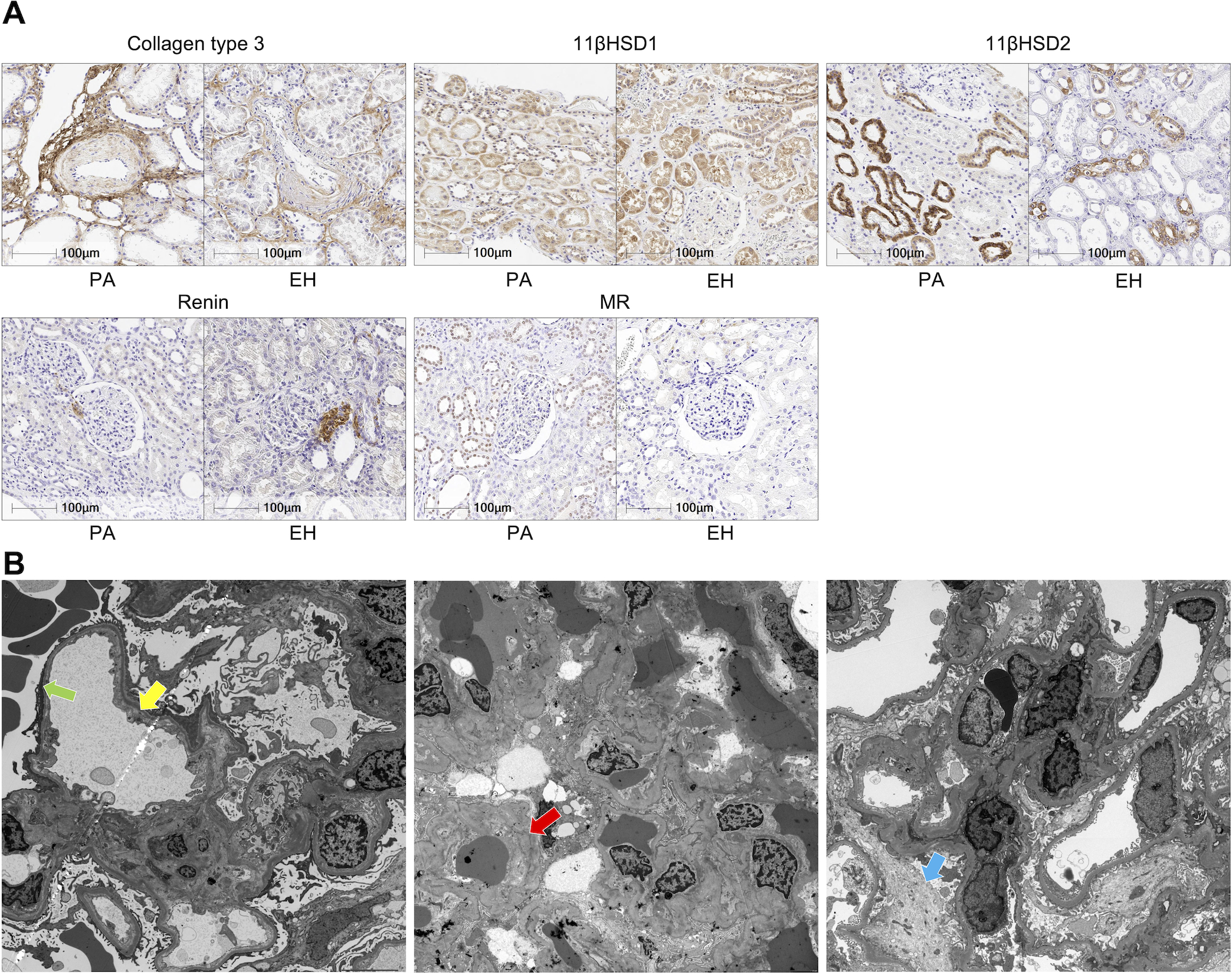
A. Representative illustrations of immunohistochemistry. PA appeared to harbor more dense perivascular fibrosis than EH (collagen type 3). Both had similar immunoreactivity of 11βHSD1. 11βHSD2 was detected mostly in distal tubules and more marked in PA. Juxtaglomerular cells were immunohistochemically positive for renin. MR nuclear immunoreactivity was detected in distal tubules but rarely in EH. B. Ultrastructural findings of 3 cases. Dilatation of subendothelial area, recognized as electron lucent lesions (yellow arrow) and foot process effacement approximately 30% of the observative area were detected (green arrow). Extra-capillary red blood cells were also detected in the left picture. Glomerular basement membrane was almost normal in the left but foci of wrinkling of basement membrane (red arrow) were detected in the middle. The latter and the right also had partial foot process effacement and slight mesangial proliferation (blue arrow). Clinical information of the cases examined was provided in Supplemental material.
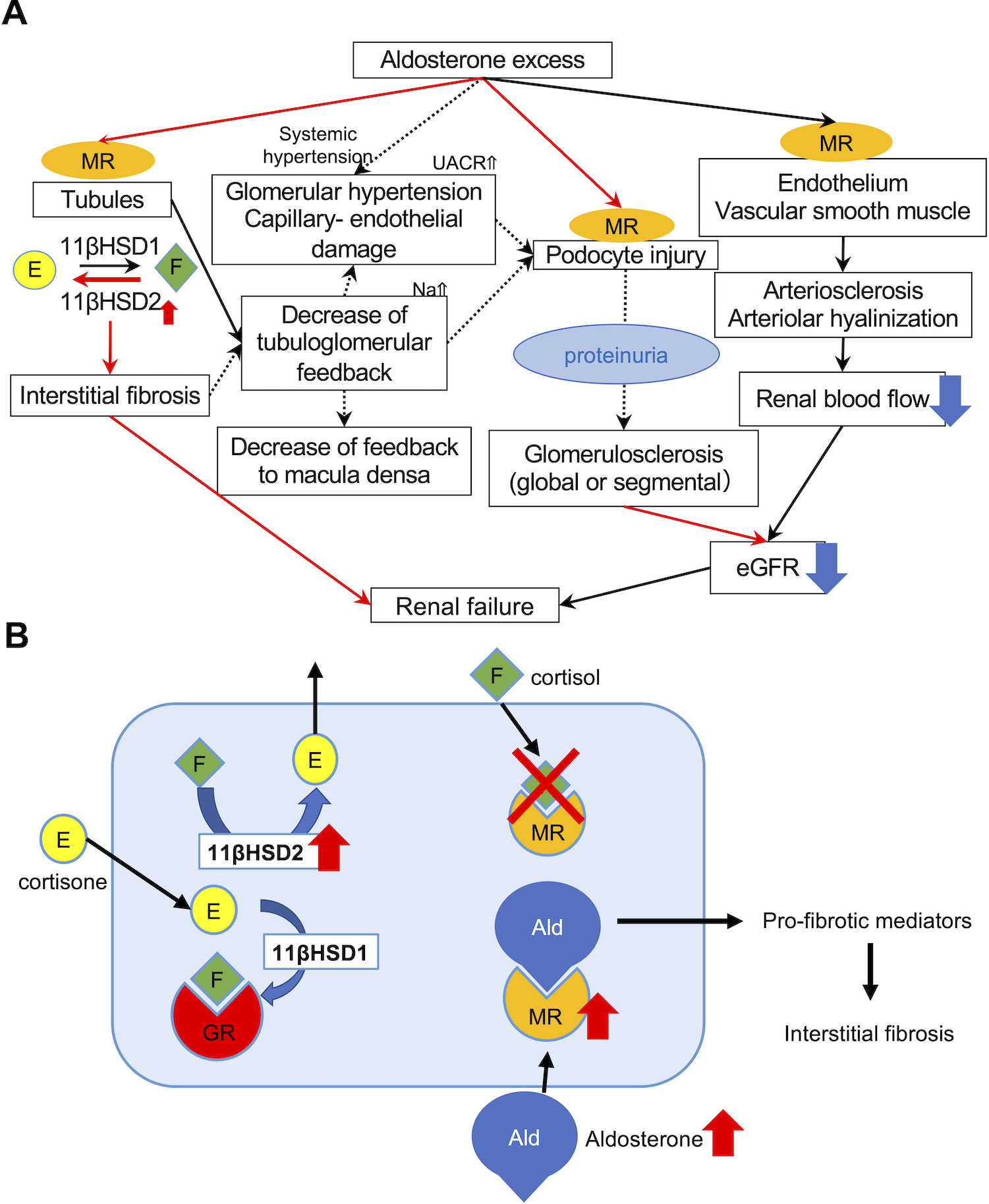
A. MR nuclear immunolocalization in PA was higher than that in EH, demonstrating that MR was more activated and translocated into nucleus as a result of abundant binding with aldosterone. Predominant 11βHSD2 catalytic status detected could compensate for aldosterone excess. Autonomous aldosterone excess (low renin and high aldosterone) could also reduce tubulo-glomerular feedback, resulting in hyperfiltrating status of the remaining glomerulus, histologically recognizable as glomerular hypertrophy. Aldosterone could also directly damage podocytes, and cause foot process effacement. Subsequently induced proteinuria also exacerbated glomerulosclerosis, histologically recognizable as progressive glomerular sclerosis demonstrated by the higher proportion of not only GGS but also SGS. In particular, the prevalence of global glomerulosclerosis accurately reflected the post-operative eGFR after adrenalectomy. Aldosterone could also influence vessels via non-genomic and genomic pathways and cause endothelial swelling and dysfunction, increasing vascular stiffness or peripheral resistance. Therefore, topical renal blood flow could be finally reduced. Therefore, aldosterone-induced renal injury could be systemically induced by multiple pathways. B. 11βHSD2 and MR immunoreactivity was more abundant in PA than EH. 11βHSD2 converted cortisol into cortisone, an inactive form of cortisol. In contrast, 11βHSD1 converted cortisone into cortisol. When 11βHSD2 was not active, MR was occupied by cortisol and aldosterone could not bind with MR. In PA, 11βHSD2-predominant status allowed aldosterone to bind MR and activate pro-fibrotic pathways.
References
-
- Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, Ganzaroli C, Giacchetti G, Letizia C, Maccario M, Mallamaci F, Mannelli M, Mattarello MJ, Moretti A, Palumbo G, Parenti G, Porteri E, Semplicini A, Rizzoni D, Rossi E, Boscaro M, Pessina AC, Mantero F; for PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1125 hypertensive patients. J Am Coll Cardiol. 2006;48(11):2293–2300. doi: 10.1016/j.jacc.2006.07.059. - DOI - PubMed
-
- Williams JS, Williams GH, Raji A, Jeunemaitre X, Brown NJ, Hopkins PN, Conlin PR. Prevalence of primary hyperaldosteronism in mild to moderate hypertension without hypokalemia. J Hum Hypertens. 2006; 20: 129–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
