

Endoscopic and Microscopic Interlaminar Discectomy for the Treatment of Far-Migrated Lumbar Disc Herniation: A Retrospective Study with a 24-Month Follow-Up
- PMID: 34121844
- PMCID: PMC8189696
- DOI: 10.2147/JPR.S302717
Endoscopic and Microscopic Interlaminar Discectomy for the Treatment of Far-Migrated Lumbar Disc Herniation: A Retrospective Study with a 24-Month Follow-Up
Abstract
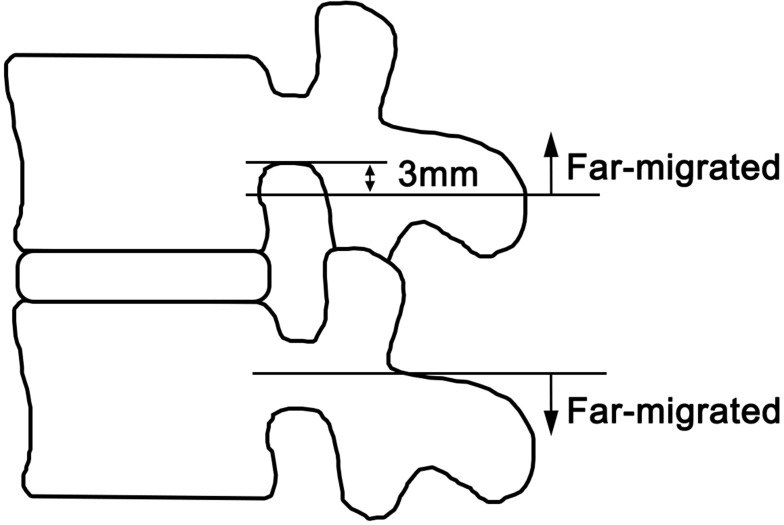
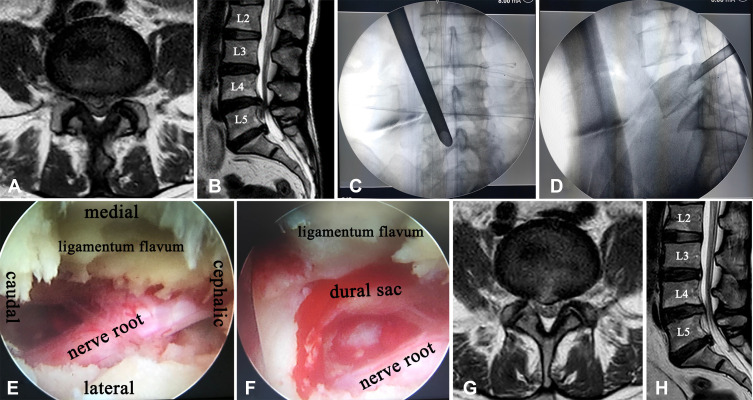
Purpose: Percutaneous endoscopic lumbar discectomy for the treatment of far-migrated lumbar disc herniation (LDH) is clinically challenging. The aim of this study was to compare the efficacy and safety of interlaminar endoscopic lumbar discectomy (IELD) and interlaminar microscopic lumbar discectomy (IMLD) for the treatment of far-migrated LDH.
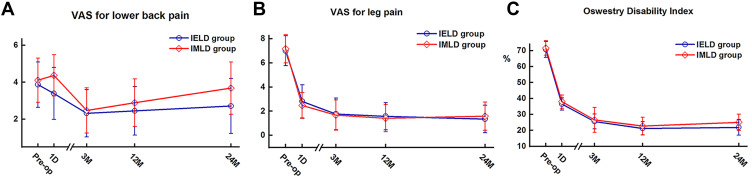
Materials and methods: We retrospectively analyzed 50 consecutive cases of far-migrated LDH treated by IELD or IMLD. Clinical data and outcomes were assessed before the operation and 1 day and 3, 12, and 24 months after the surgery using the visual analog scale (VAS) and Oswestry disability index (ODI). Modified MacNab criteria were used to evaluate patient satisfaction at the 24-month follow-up.
Results: A significant reduction in leg pain and improvement in ODI (P<0.01) were observed in both groups after surgery. Lower back pain (LBP) was reduced at 24 months postsurgery in the IELD group (P<0.05) but not in the IMLD group (P>0.05). There were significant intergroup differences in VAS LBP score at 1 day and 24 months postsurgery (p=0.01 and 0.02, respectively) and in ODI at 24 months (p=0.03). The rate of excellent or good outcome was 90.32% with IELD and 78.95% with IMLD (p=0.55). Hospital stay and time to ambulation were shorter in the IELD group than in the IMLD group, but the former had a longer operative time (p<0.01). Low and comparable complication rates were reported in the IELD (16.13%) and IMLD (10.53%) groups (p=0.70).
Conclusion: Both IELD and IMLD achieve favorable clinical results in the treatment of far-migrated LDH, with only minor complications. Compared to IMLD, LBP was significantly reduced with IELD presumably because it involved less trauma.
Keywords: downward migration; highly migrated lumbar disc herniation; interlaminar approach; minimally invasive spinal surgery; upward migration.
© 2021 Yang et al.
Conflict of interest statement
The authors report no conflicts of interest for this work nor concerning the materials or methods related to the findings described in this paper.
Figures
Similar articles
-
Comparative analysis of endoscopic discectomy for demanding lumbar disc herniation.Sci Rep. 2025 Mar 17;15(1):9098. doi: 10.1038/s41598-025-91964-3. Sci Rep. 2025. PMID: 40097536 Free PMC article.
-
Early Clinical Outcomes of Percutaneous Endoscopic Lumbar Discectomy for L4-5 Highly Down-Migrated Disc Herniation: Interlaminar Approach Versus Transforaminal Approach.World Neurosurg. 2021 Feb;146:e413-e418. doi: 10.1016/j.wneu.2020.10.105. Epub 2020 Oct 24. World Neurosurg. 2021. PMID: 33353758
-
Percutaneous Endoscopic Lumbar Discectomy via Transforaminal Approach Combined with Interlaminar Approach for L4/5 and L5/S1 Two-Level Disc Herniation.Orthop Surg. 2021 May;13(3):979-988. doi: 10.1111/os.12862. Epub 2021 Apr 5. Orthop Surg. 2021. PMID: 33821557 Free PMC article.
-
Transforaminal Versus Interlaminar Endoscopic Lumbar Discectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis.Global Spine J. 2023 Mar;13(2):575-587. doi: 10.1177/21925682221120530. Epub 2022 Aug 21. Global Spine J. 2023. PMID: 35993298 Free PMC article. Review.
-
Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: a meta-analysis.Int Orthop. 2019 Apr;43(4):923-937. doi: 10.1007/s00264-018-4253-8. Epub 2018 Dec 13. Int Orthop. 2019. PMID: 30547214
Cited by
-
Percutaneous endoscopic interlaminar discectomy for high-grade migrated lumbar disc herniation: clinical efficacy and safety assessment.Int Orthop. 2024 Sep;48(9):2455-2463. doi: 10.1007/s00264-024-06246-w. Epub 2024 Jul 6. Int Orthop. 2024. PMID: 38969821
-
One-hole split endoscope technique for migrated lumbar disc herniation: a single-centre, retrospective study of a novel technique.J Orthop Surg Res. 2023 Jul 5;18(1):483. doi: 10.1186/s13018-023-03967-3. J Orthop Surg Res. 2023. PMID: 37408054 Free PMC article.
-
Microendoscopic lumbar discectomy with general versus local anesthesia: A systematic review and meta-analysis.N Am Spine Soc J. 2022 May 30;10:100129. doi: 10.1016/j.xnsj.2022.100129. eCollection 2022 Jun. N Am Spine Soc J. 2022. PMID: 35712327 Free PMC article. Review.
-
Comparative analysis of endoscopic discectomy for demanding lumbar disc herniation.Sci Rep. 2025 Mar 17;15(1):9098. doi: 10.1038/s41598-025-91964-3. Sci Rep. 2025. PMID: 40097536 Free PMC article.
-
Large-Channel Interlaminar Endoscopic Discectomy for Highly Migrated Lumbar Disc Herniation: Effectiveness and Safety.J Pain Res. 2025 Aug 1;18:3821-3832. doi: 10.2147/JPR.S537181. eCollection 2025. J Pain Res. 2025. PMID: 40766100 Free PMC article.
References
-
- Anderson G. Epidemiology of spinal disorders. In: Frymoyer JW, Ducker TB, Hadler NM, editors. The Adult Spine: Principles and Practice. New York: Raven Press; 1997:93–141.
LinkOut - more resources
Full Text Sources
Miscellaneous
