

Mapping of the Language Cortex
- PMID: 34123657
- PMCID: PMC8191642
- DOI: 10.7759/cureus.14960
Mapping of the Language Cortex
Abstract
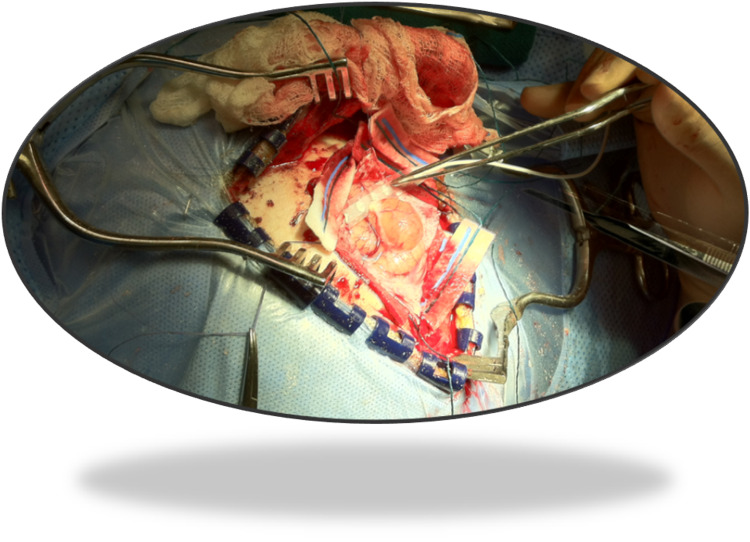
Awake craniotomy with intraoperative neurophysiological language mapping (INLM) is an established procedure for patients undergoing surgery to resection tumors in the language cortex area. INLM and continuous neurophysiological monitoring allow assessment of the language function, which is not possible under general anesthesia. INLM of the brain areas provides a helpful tool to the operating surgeon in reducing the risks associated with tumor resection in the motor and language cortex. We present a literature review and the technical method used for INLM by utilizing direct electrical cortical stimulation. We also report the usefulness of INLM for evaluation of the language function during resection of cortical tumors, epilepsy foci, and arteriovenous malformations (AVMs) located near language areas. First, the central sulcus is identified by sensory mapping, followed by the motor cortex's identification by direct electrical cortical stimulation (DECS). Neurological assessment of the patient is done by auditory and visual feedback. The patient is asked to repeat numbers, days, words, sentences, read words, and name pictures during cortical stimulation. DECS may cause a slurring or speech arrest. Electrocorticography (ECoG) is also performed during cortical stimulation to identify any after-discharges. Examination of the patient occurs immediately after surgery, and then 24 hours, one week, six months, and 12 months postoperatively. Bipolar DECS for motor mapping with ECoG can safely and reliably be utilized to identify essential language areas with minimizing permanent language deficits and maximizing the extent of tumor resection.
Keywords: broca’s; cortical mapping; eloquent area; ionm; language mapping; neuromonitoring; neurophysiology; tumors; wernicke’s.
Copyright © 2021, Jahangiri et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
-
- Dineen J, Nahed BV, Simon MV. Intraoperative Neurophysiology: A Comprehensive Guide to Monitoring and Mapping. Vol. 2. Springer; 2019. Mapping and monitoring of language and parietal functions; pp. 284–302.
-
- The asleep-awake-asleep anesthetic technique for intraoperative language mapping. Huncke K, Van de Wiele B, Fried I, Rubinstein EH. Neurosurgery. 1998;42:1312–1316. - PubMed
-
- Variability of intraoperative electrocortical stimulation mapping parameters across and within individuals. Pouratian N, Cannestra AF, Bookheimer SY, Martin NA, Toga AW. J Neurosurg. 2004;101:458–466. - PubMed
-
- Jahangiri FR. Charleston: CreateSpace; 2012. Surgical Neurophysiology: A Reference Guide to Intraoperative Neurophysiological Monitoring (IONM), 2nd Edition. - PubMed
LinkOut - more resources
Full Text Sources