

Interposition arthroplasty: Current indications, technique and expectations
- PMID: 34123723
- PMCID: PMC8170494
- DOI: 10.1016/j.jcot.2021.05.023
Interposition arthroplasty: Current indications, technique and expectations
Erratum in
-
Erratum regarding previously published articles.J Clin Orthop Trauma. 2021 Jul 30;20:101540. doi: 10.1016/j.jcot.2021.101540. eCollection 2021 Sep. J Clin Orthop Trauma. 2021. PMID: 34405085 Free PMC article.
Abstract
The ultimate means of functional restoration of joints with end stage arthritis is prosthetic replacement. Even though there is reluctance to replace the joint of a younger individual, the mean age of joint replacement continues to decrease. This is due to three factors: 1) social expectations, 2) uncertainty with many joint preservation procedures and 3) the ever-increasing reliability and longevity of prosthetic replacement. Unfortunately, the elbow does not share in these advantageous trends to the extent as is the case for the hip, knee and shoulder. Social pressure for restoration of normal or near normal function is certainly present, but the desired improvement of longevity and fewer restrictions of activity have not been documented. Hence, possibly somewhat disproportionately to other joints, there is great need for a reliable and functional non replacement joint reconstruction option. For most other joints, fusion is the ultimate non replacement option. Further, for most joints an optimum position has been defined to allow the greatest chance of normal function of the individual. Unfortunately, there is no truly 'optimum' functional position of elbow fusion, and the recommended 90° of flexion is considered the 'least worse' position. Further, unfortunately, elbow fusion dysfunction cannot be mitigated by compensated shoulder motion. Hence, while there is little experience in general with interposition arthroplasty of the elbow, in the authors' opinion it remains the treatment of choice in some individuals and in certain circumstances for the reasons explained above. In our judgment, the reason for avoiding this procedure is that it is technically difficult, the absolute frequency of need is not great, and outcomes do appear to be a function of experience and technique. Based on these considerations, in this chapter we review the current indications and assessment and selection considerations. Emphasis is placed on our current technique with technical tips to enhance the likelihood of success and longevity. We conclude with a review of expectations based on current literature.
© 2021.
Figures

References
-
- O'Neill O.R., Morrey B.F., Tanaka S., An K.N. Compensatory motion in the upper extremity after elbow arthrodesis. Clin Orthop. 1992;281:89–96. PMID:1499233, 8. - PubMed
-
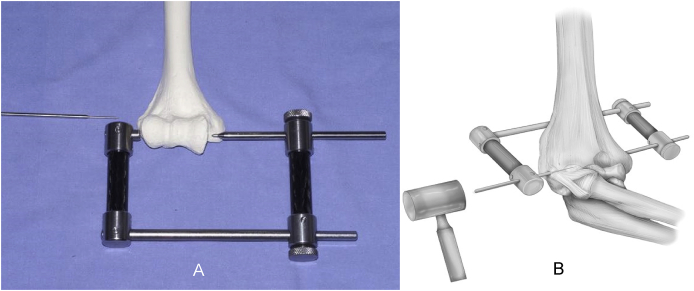
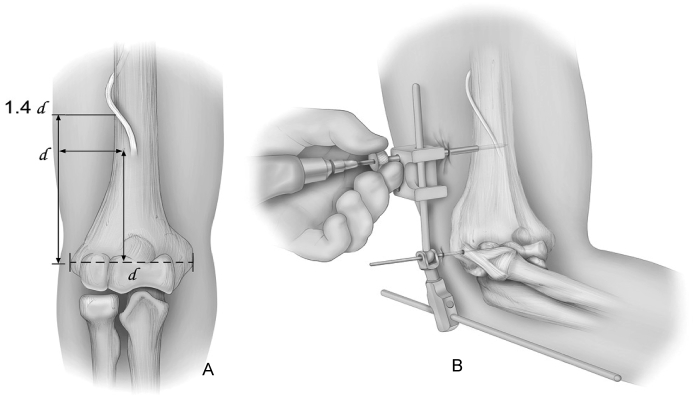
- Morrey B.F. Interposition arthroplasty. Chap 114. In: Morrey B., Sanchez Sotelo J., Morrey M., editors. The Elbow and It's Disorders. fifth ed.. Elsevier; 2018.
-
- Cheng S.L., Morrey B.F. Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br. 2000;82(2):233–238. Mar. PMID:10755432. - PubMed
LinkOut - more resources
Full Text Sources