

Prevalence of SARS-CoV-2 in urban and rural Ethiopia: Randomized household serosurveys reveal level of spread during the first wave of the pandemic
- PMID: 34124630
- PMCID: PMC8176122
- DOI: 10.1016/j.eclinm.2021.100880
Prevalence of SARS-CoV-2 in urban and rural Ethiopia: Randomized household serosurveys reveal level of spread during the first wave of the pandemic
Abstract
Background: The spread of SARS-CoV-2 in Sub-Saharan Africa is poorly understood and to date has generally been characterised by a lower number of declared cases and deaths as compared to other regions of the world. Paucity of reliable information, with insights largely derived from limited RT-PCR testing in high-risk and urban populations, has been one of the biggest barriers to understanding the course of the pandemic and informed policy-making. Here we estimate seroprevalence of anti-SARS-CoV-2 antibodies in Ethiopia during the first wave of the pandemic.
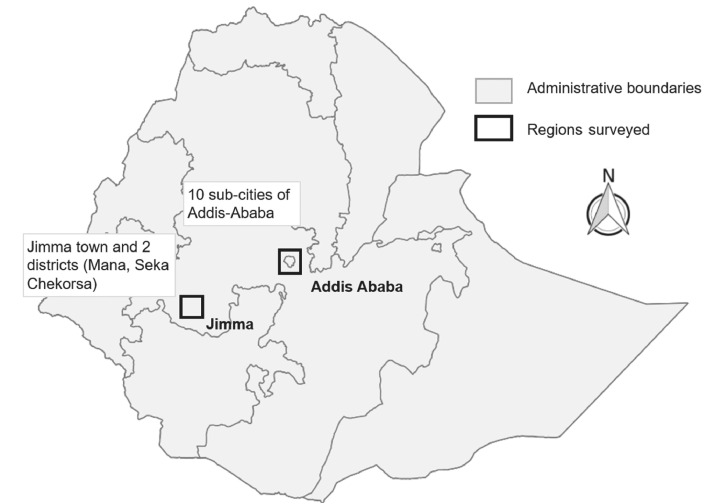
Methods: We undertook a population-based household seroprevalence serosurvey based on 1856 participants in Ethiopia, in the capital city Addis Ababa, and in Jimma, a middle-sized town in the Oromia region, and its rural surroundings (districts of Seka and Mana), between 22 July and 02 September 2020. We tested one random participant per household for anti-SARS-CoV-2 antibodies using a high specificity rapid diagnostic tests (RDTs) and evaluated population seroprevalence using a Bayesian logistic regression model taking into account test performance as well as age and sex of the participants.
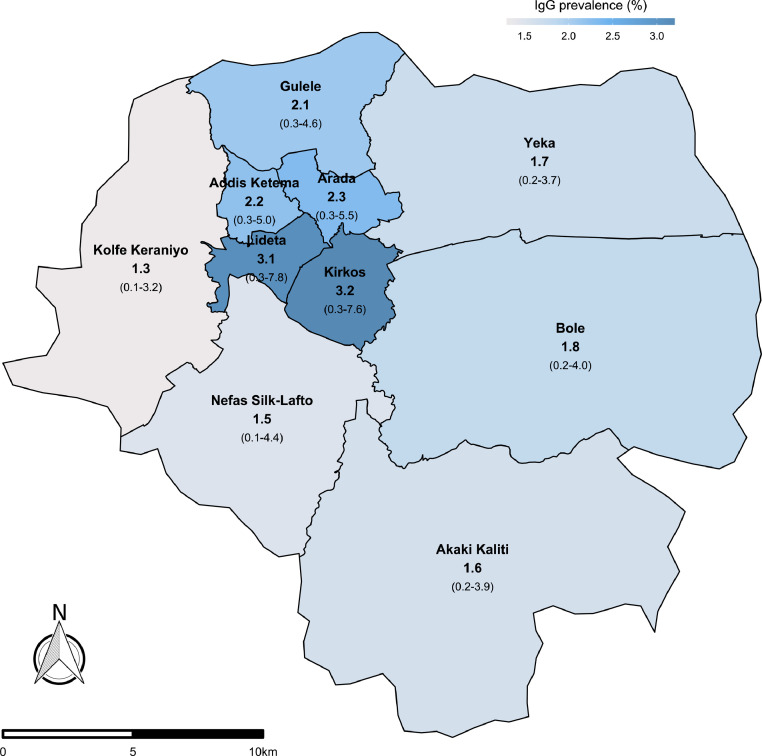
Findings: In total, 2304 random households were visited, with 1856 individuals consenting to participate. This produced a sample of 956 participants in Addis Ababa and 900 participants in Jimma. IgG prevalence was estimated at 1.9% (95% CI 0.4-3.7%), and combined IgM/IgG prevalence at 3.5% (95% CI 1.7-5.4%) for Addis Ababa in early August 2020, with higher prevalence in central sub-cities. Prevalence in Jimma town was lower at 0.5% (95% CI 0-1.8%) for IgG and 1.6% (95%CI 0-4.1%) for IgM/IgG, while in rural Jimma IgG prevalence was 0.2% and IgM/IgG 0.4% in early September.
Interpretation: More than four months after the first cases were detected in Ethiopia, Addis Ababa displayed a prevalence under 5% and likely as low as 2%, while rural Jimma displayed a prevalence of 0.2%. A 2% seroprevalence figure for the capital translated to a number of cases at least five times larger than those reported for the country as a whole. At the same time, it contrasts with significantly higher seroprevalence figures in large cities in Europe and America only two to three months after the first cases. This population-based seroepidemiological study thus provides evidence of a slower spread of SARS-CoV-2 in the Ethiopian population during the first wave of the pandemic and does not appear to support the notion that lower case numbers were simply a reflection of limited testing and surveillance.
Funding: Schmidt Family Foundation, Joachim Hertz Foundation, Nespresso, Peet's and Smuckers.
Keywords: Africa; Ethiopia; Household surveys; Prevalence; SARS-CoV-2.
© 2021 The Author(s).
Conflict of interest statement
We declare no competing interests.
Figures
References
-
- ECDC . European Center for Disease Control; 2020. Daily number of new reported cases of COVID-19 by country worldwide.https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geo... published online Nov 22. (accessed Nov 23, 2020)
-
- Mbow M., Lell B., Jochems S.P. COVID-19 in Africa: dampening the storm? Science. 2020;369:624–626. - PubMed
-
- Maeda J.M., Nkengasong J.N. The puzzle of the COVID-19 pandemic in Africa. Science. 2021;371:27–28. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
