

Inflammatory biomarkers in COVID-19-associated multisystem inflammatory syndrome in children, Kawasaki disease, and macrophage activation syndrome: a cohort study
- PMID: 34124694
- PMCID: PMC8186852
- DOI: 10.1016/S2665-9913(21)00139-9
Inflammatory biomarkers in COVID-19-associated multisystem inflammatory syndrome in children, Kawasaki disease, and macrophage activation syndrome: a cohort study
Abstract
Background: Multisystem inflammatory syndrome in children (MIS-C) is a potentially life-threatening hyperinflammatory syndrome that occurs after primary SARS-CoV-2 infection. The pathogenesis of MIS-C remains undefined, and whether specific inflammatory biomarker patterns can distinguish MIS-C from other hyperinflammatory syndromes, including Kawasaki disease and macrophage activation syndrome (MAS), is unknown. Therefore, we aimed to investigate whether inflammatory biomarkers could be used to distinguish between these conditions.
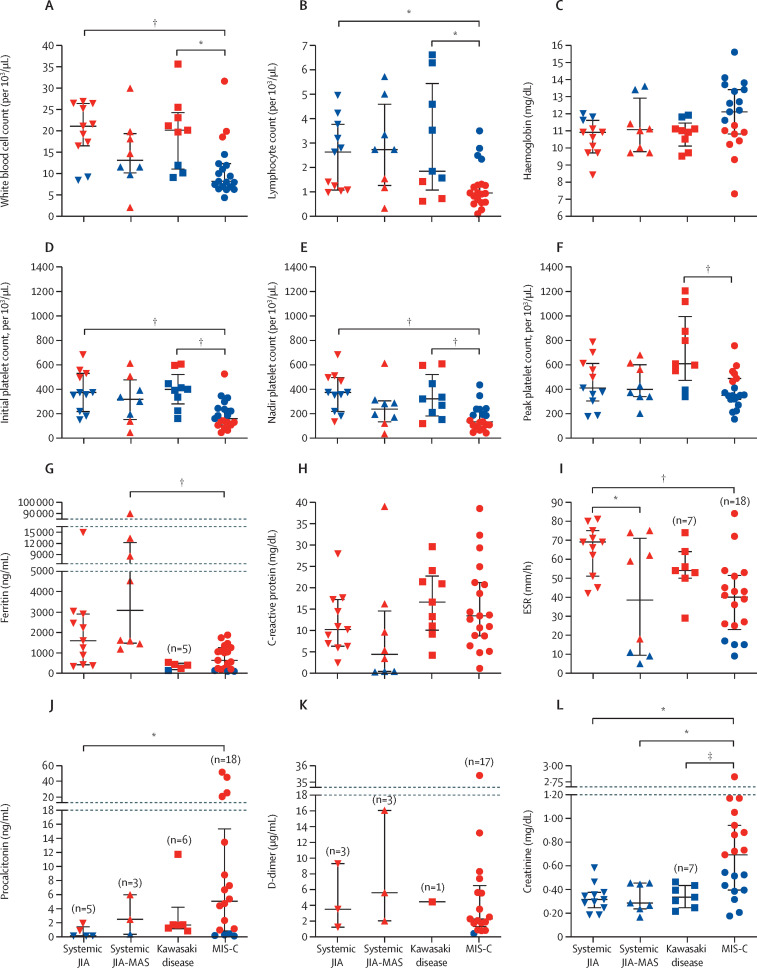
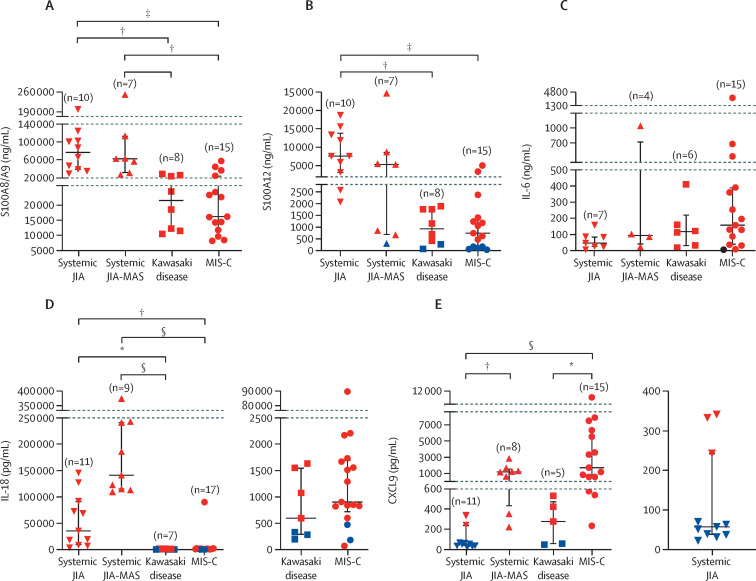
Methods: We studied a prospective cohort of patients with MIS-C and Kawasaki disease and an established cohort of patients with new-onset systemic juvenile idiopathic arthritis (JIA) and MAS associated with systemic JIA (JIA-MAS), diagnosed according to established guidelines. The study was done at Cincinnati Children's Hospital Medical Center (Cincinnati, OH, USA). Clinical and laboratory features as well as S100A8/A9, S100A12, interleukin (IL)-18, chemokine (C-X-C motif) ligand 9 (CXCL9), and IL-6 concentrations were assessed by ELISA and compared using parametric and non-parametric tests and receiver operating characteristic curve analysis.
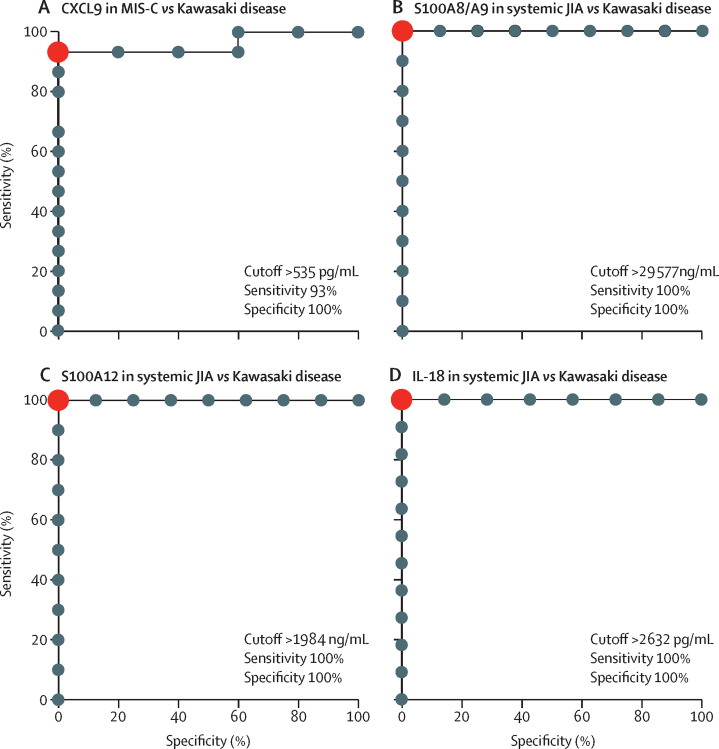
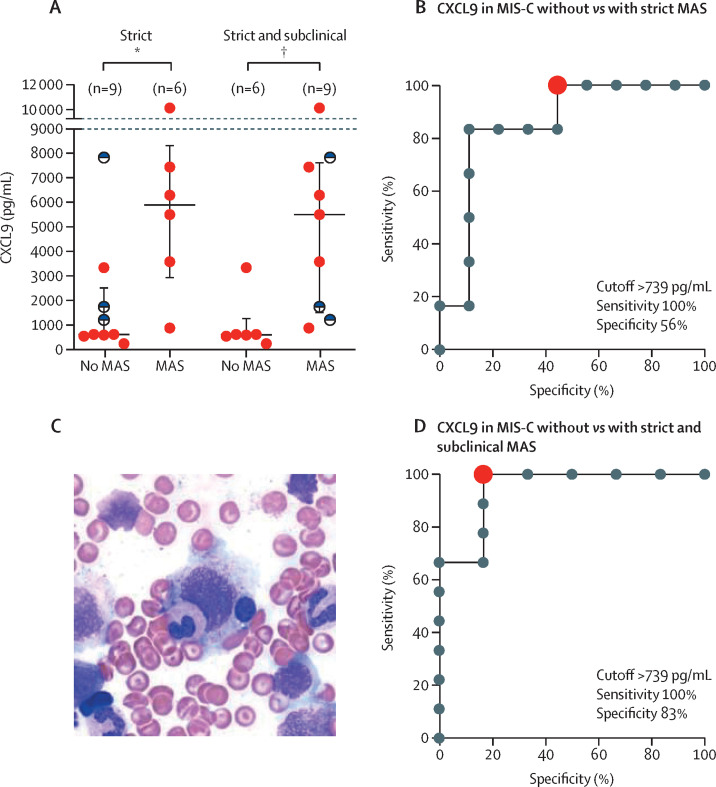
Findings: Between April 30, 2019, and Dec 14, 2020, we enrolled 19 patients with MIS-C (median age 9·0 years [IQR 4·5-15·0]; eight [42%] girls and 11 [58%] boys) and nine patients with Kawasaki disease (median age 2·0 years [2·0-4·0]); seven [78%] girls and two [22%] boys). Patients with MIS-C and Kawasaki disease had similar S100 proteins and IL-18 concentrations but patients with MIS-C were distinguished by significantly higher median concentrations of the IFNγ-induced CXCL9 (1730 pg/mL [IQR 604-6300] vs 278 pg/mL [54-477]; p=0·038). Stratifying patients with MIS-C by CXCL9 concentrations (high vs low) revealed differential severity of clinical and laboratory presentation. Compared with patients with MIS-C and low CXCL9 concentrations, more patients with high CXCL9 concentrations had acute kidney injury (six [60%] of ten vs none [0%] of five), altered mental status (four [40%] of ten vs none [0%] of five), shock (nine [90%] of ten vs two [40%] of five), and myocardial dysfunction (five [50%] of ten vs one [20%] of five); these patients also had higher concentrations of systemic inflammatory markers and increased severity of cytopenia and coagulopathy. By contrast, patients with MIS-C and low CXCL9 concentrations resembled patients with Kawasaki disease, including the frequency of coronary involvement. Elevated concentrations of S100A8/A9, S100A12, and IL-18 were also useful in distinguishing systemic JIA from Kawasaki disease with high sensitivity and specificity.
Interpretation: Our findings show MIS-C is distinguishable from Kawasaki disease primarily by elevated CXCL9 concentrations. The stratification of patients with MIS-C by high or low CXCL9 concentrations provides support for MAS-like pathophysiology in patients with severe MIS-C, suggesting new approaches for diagnosis and management.
Funding: Cincinnati Children's Research Foundation, National Institute of Arthritis and Musculoskeletal and Skin Diseases/National Institutes of Health, the Deutsche Forschungsgemeinschaft, and The Jellin Family Foundation.
© 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
AG has served as a consultant and received research support from Novartis, SOBI, NovImmune, and AB2Bio. GS reports consulting fees from Novartis and SOBI. All other authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
