Association Between Childhood Consumption of Ultraprocessed Food and Adiposity Trajectories in the Avon Longitudinal Study of Parents and Children Birth Cohort
- PMID: 34125152
- PMCID: PMC8424476
- DOI: 10.1001/jamapediatrics.2021.1573
Association Between Childhood Consumption of Ultraprocessed Food and Adiposity Trajectories in the Avon Longitudinal Study of Parents and Children Birth Cohort
Abstract
Importance: Reports of associations between higher consumption of ultraprocessed foods (UPF) and elevated risks of obesity, noncommunicable diseases, and mortality in adults are increasing. However, associations of UPF consumption with long-term adiposity trajectories have never been investigated in children.
Objective: To assess longitudinal associations between UPF consumption and adiposity trajectories from childhood to early adulthood.
Design, setting, and participants: This prospective birth cohort study included children who participated in the Avon Longitudinal Study of Parents and Children (ALSPAC) in Avon County, southwest England. Children were followed up from 7 to 24 years of age during the study period from September 1, 1998, to October 31, 2017. Data were analyzed from March 1, 2020, to January 31, 2021.
Exposures: Baseline dietary intake data were collected using 3-day food diaries. Consumption of UPF (applying the NOVA food classification system) was computed as a percentage of weight contribution in the total daily food intake for each participant and categorized into quintiles.
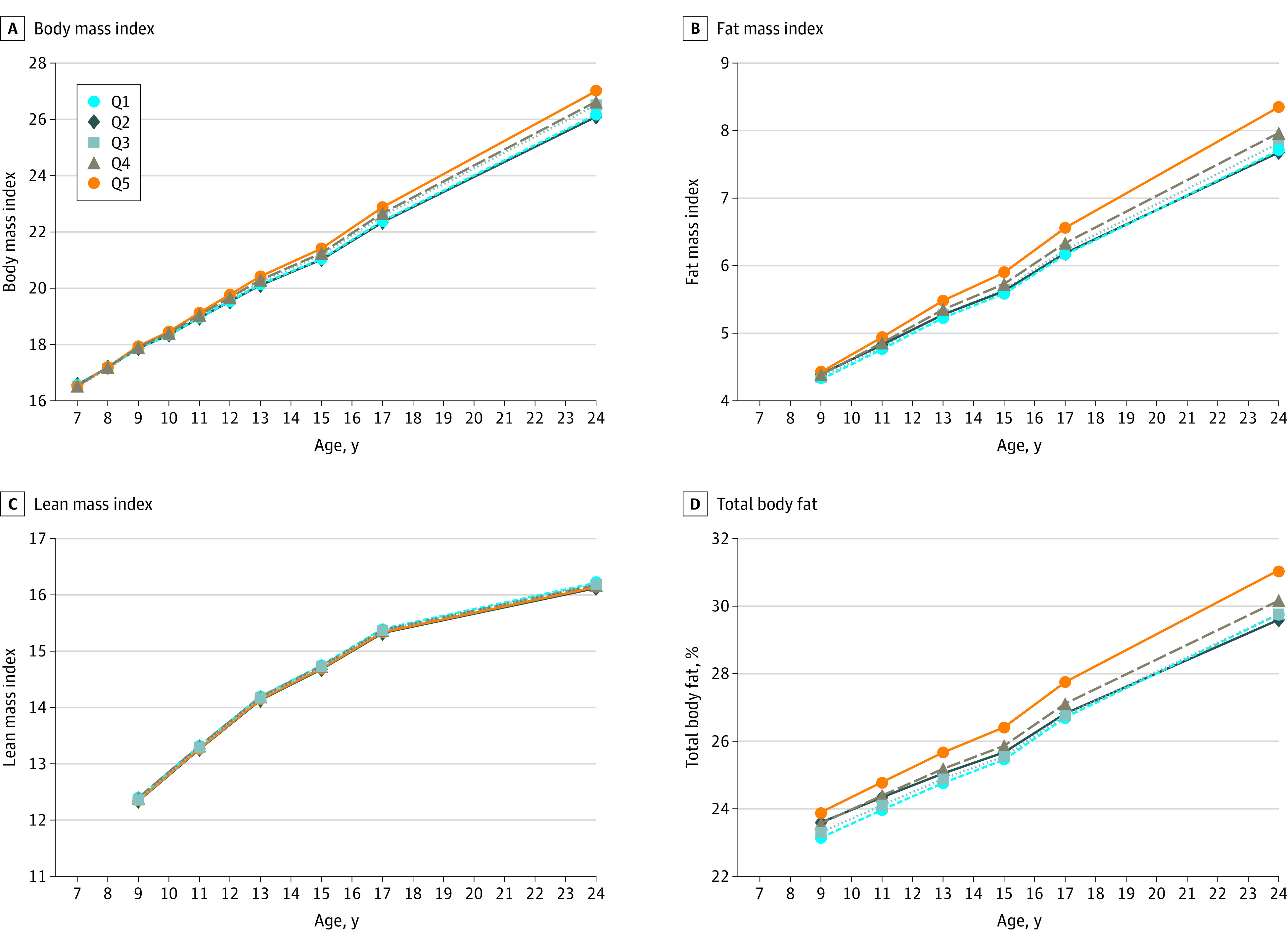
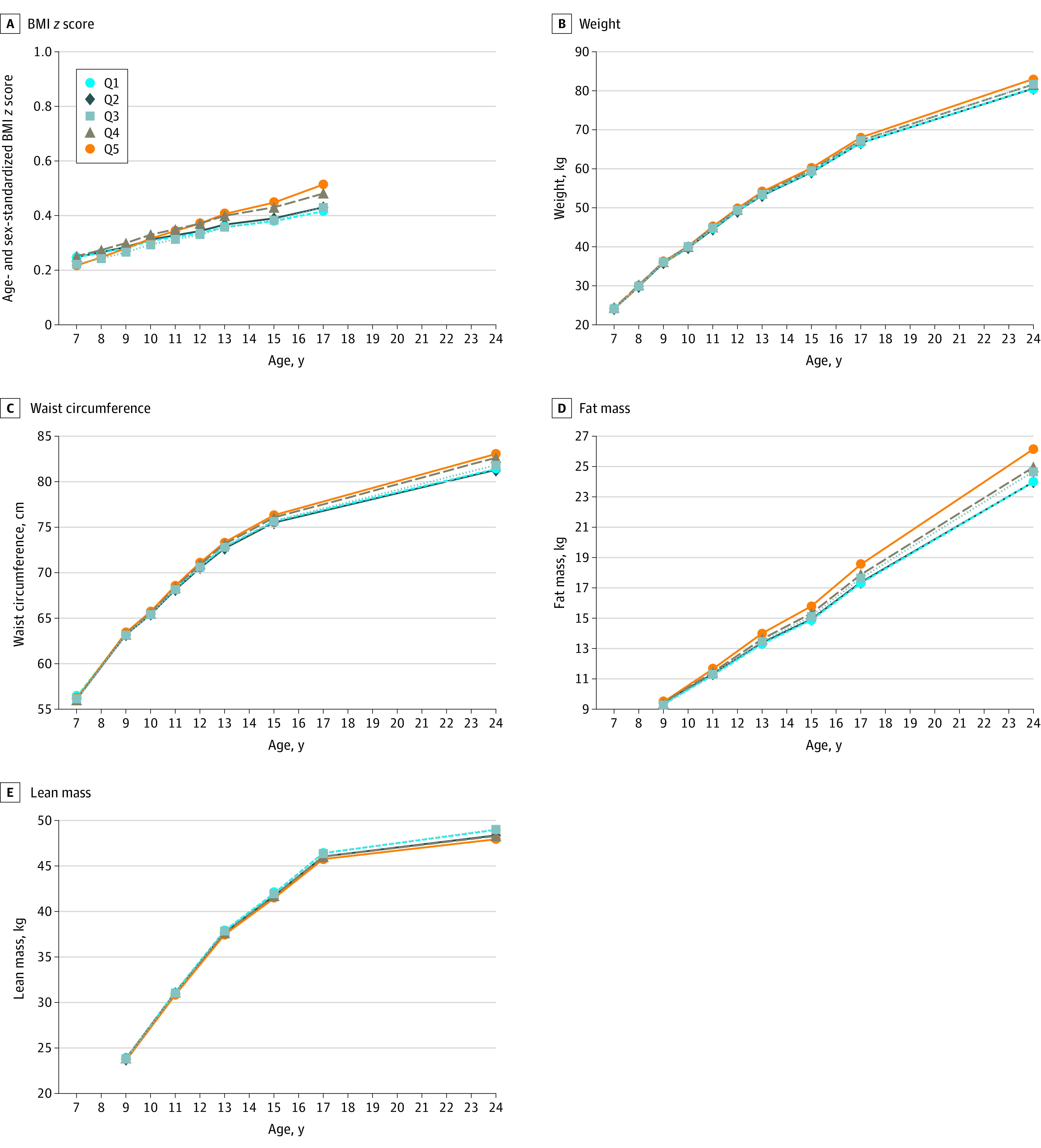
Main outcomes and measures: Repeated recordings of objectively assessed anthropometrics (body mass index [BMI; calculated as weight in kilograms divided by height in meters squared], weight, and waist circumference) and dual-energy x-ray absorptiometry measurements (fat and lean mass indexes [calculated as fat and lean mass, respectively, divided by height in meters squared] and body fat percentage). Associations were evaluated using linear growth curve models and were adjusted for study covariates.
Results: A total of 9025 children (4481 [49.7%] female and 4544 [50.3%] male) were followed up for a median of 10.2 (interquartile range, 5.2-16.4) years. The mean (SD) UPF consumption at baseline was 23.2% (5.0%) in quintile 1, 34.7% (2.5%) in quintile 2, 43.4% (2.5%) in quintile 3, 52.7% (2.8%) in quintile 4, and 67.8% (8.1%) in quintile 5. Among those in the highest quintile of UPF consumption compared with their lowest quintile counterpart, trajectories of BMI increased by an additional 0.06 (95% CI, 0.04-0.08) per year; fat mass index, by an additional 0.03 (95% CI, 0.01-0.05) per year; weight, by an additional 0.20 (95% CI, 0.11-0.28) kg per year; and waist circumference, by an additional 0.17 (95% CI, 0.11-0.22) cm per year.
Conclusions and relevance: These findings suggest that higher UPF consumption is associated with greater increases in adiposity from childhood to early adulthood. Robust public health measures that promote minimally processed foods and discourage UPF consumption among children are urgently needed to reduce obesity in England and globally.
Conflict of interest statement
Figures