

Prevalence and risk factors of hemodynamic instability associated with preload-dependence during continuous renal replacement therapy in a prospective observational cohort of critically ill patients
- PMID: 34125314
- PMCID: PMC8200783
- DOI: 10.1186/s13613-021-00883-9
Prevalence and risk factors of hemodynamic instability associated with preload-dependence during continuous renal replacement therapy in a prospective observational cohort of critically ill patients
Abstract
Background: Hemodynamic instability is a frequent complication of continuous renal replacement therapy (CRRT). Postural tests (i.e., passive leg raising in the supine position or Trendelenburg maneuver in the prone position) combined with measurement of cardiac output are highly reliable to identify preload-dependence and may provide new insights into the mechanisms involved in hemodynamic instability related to CRRT (HIRRT). We aimed to assess the prevalence and risk factors of HIRRT associated with preload-dependence in ICU patients. We conducted a single-center prospective observational cohort study in ICU patients with acute kidney injury KDIGO 3, started on CRRT in the last 24 h, and monitored with a PiCCO® device. The primary endpoint was the rate of HIRRT episodes associated with preload-dependence during the first 7 days after inclusion. HIRRT was defined as the occurrence of a mean arterial pressure below 65 mmHg requiring therapeutic intervention. Preload-dependence was assessed by postural tests every 4 h, and during each HIRRT episode. Data are expressed in median [1st quartile-3rd quartile], unless stated otherwise.
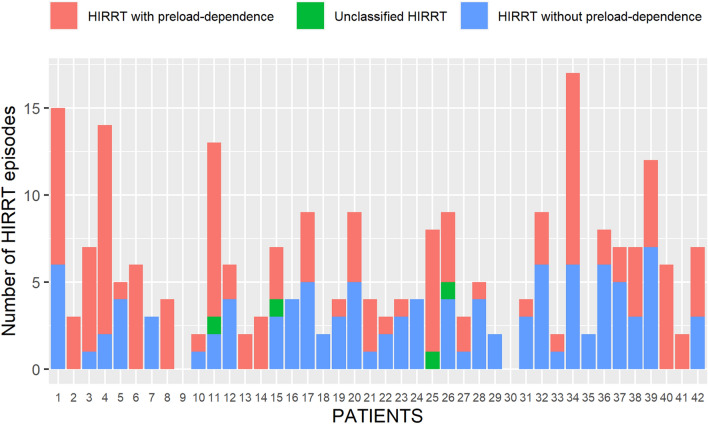
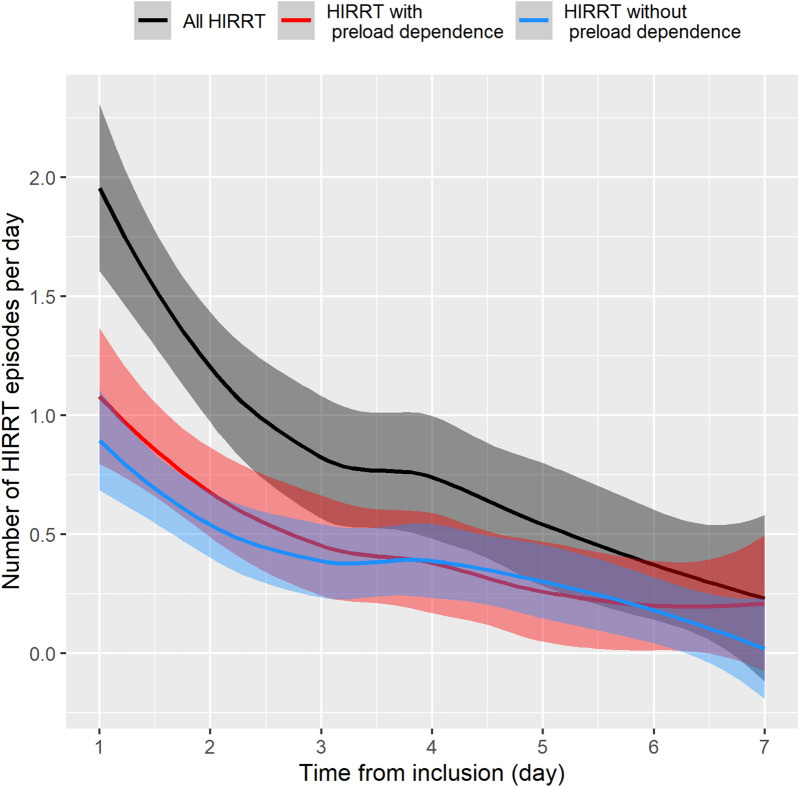
Results: 42 patients (62% male, age 69 [59-77] year, SAPS-2 65 [49-76]) were included 6 [1-16] h after CRRT initiation and studied continuously for 121 [60-147] h. A median of 5 [3-8] HIRRT episodes occurred per patient, for a pooled total of 243 episodes. 131 episodes (54% [CI95% 48-60%]) were associated with preload-dependence, 108 (44%, [CI95% 38-51%]) without preload-dependence, and 4 were unclassified. Multivariate analysis (using variables collected prior to HIRRT) identified the following variables as risk factors for the occurrence of HIRRT associated with preload-dependence: preload-dependence before HIRRT [odds ratio (OR) = 3.82, p < 0.001], delay since last HIRRT episode > 8 h (OR = 0.56, p < 0.05), lactate (OR = 1.21 per 1-mmol L-1 increase, p < 0.05), cardiac index (OR = 0.47 per 1-L min-1 m-2 increase, p < 0.001) and SOFA at ICU admission (OR = 0.91 per 1-point increase, p < 0.001). None of the CRRT settings was identified as risk factor for HIRRT.
Conclusions: In this single-center study, HIRRT associated with preload-dependence was slightly more frequent than HIRRT without preload-dependence in ICU patients undergoing CRRT. Testing for preload-dependence could help avoiding unnecessary decrease of fluid removal in preload-independent HIRRT during CRRT.
Keywords: Acute circulatory failure; Acute kidney injury; Hemodynamic instability; Net ultrafiltration rate; Preload-dependence; Pulse contour; Renal replacement therapy; Thermodilution.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- RENAL Replacement Therapy Study Investigators. Bellomo R, Cass A, Cole L, Finfer S, Gallagher M, et al. An observational study fluid balance and patient outcomes in the randomized evaluation of normal vs. augmented level of replacement therapy trial. Crit Care Med. 2012;40:1753–1760. doi: 10.1097/CCM.0b013e318246b9c6. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
