

Vulvar Melanoma: Molecular Characteristics, Diagnosis, Surgical Management, and Medical Treatment
- PMID: 34125416
- PMCID: PMC8421300
- DOI: 10.1007/s40257-021-00614-7
Vulvar Melanoma: Molecular Characteristics, Diagnosis, Surgical Management, and Medical Treatment
Abstract
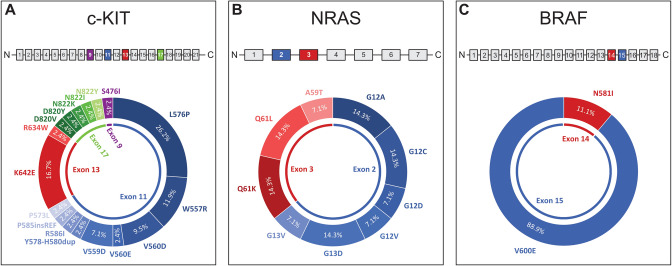
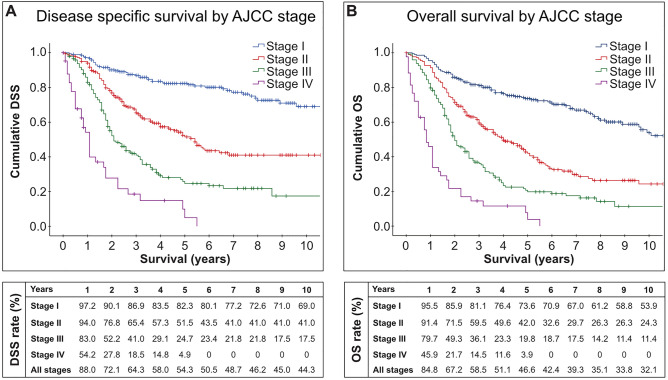
Ten percent of all women have pigmented vulvar lesions. Fortunately, most of these are benign but 1% of all melanomas in women affect the vulva. While the mortality rate of cutaneous melanoma has dropped by 7% annually during the last 5 years, the prognosis of vulvar melanoma remains dismal: the 5-year overall survival rate is 47% compared with 92% for cutaneous melanoma. The current evidence suggests that this likely results from a combination of delayed diagnosis and different tumor biology, treatment strategies, and treatment response. Although many landmark trials on checkpoint inhibitors included mucosal and vulvar melanomas, the results were often not reported separately. Post-hoc analyses indicate overall response rates between 19 and 37% for checkpoint inhibitors. A recently published retrospective study on vulvar melanomas suggests an objective response in 33.3% with a similar safety profile to cutaneous melanoma. Tyrosine kinase inhibitors may be considered in recurrent disease if a c-KIT mutation is present.
© 2021. The Author(s).
Conflict of interest statement
Christoph Wohlmuth and Iris Wohlmuth-Wieser have no conflicts of interest that are directly relevant to the content of this article.
Figures
Similar articles
-
Pigmented lesions of the vulva.Dermatol Clin. 2010 Oct;28(4):795-805. doi: 10.1016/j.det.2010.08.007. Dermatol Clin. 2010. PMID: 20883921 Review.
-
Surgical pathology, management and outcome in the vulvar melanoma associated with abdominal mass - a case report.Rom J Morphol Embryol. 2016;57(4):1375-1381. Rom J Morphol Embryol. 2016. PMID: 28174807
-
Premalignant epithelial disorders of the vulva: squamous vulvar intraepithelial neoplasia, vulvar Paget's disease and melanoma in situ.Acta Obstet Gynecol Scand. 2010 Jun;89(6):741-8. doi: 10.3109/00016341003739575. Acta Obstet Gynecol Scand. 2010. PMID: 20504079 Review.
-
Primary malignant melanoma of the vulva--an aggressive tumor for modeling the genesis of non-UV light-associated melanomas.Acta Oncol. 2004;43(5):421-35. doi: 10.1080/02841860410031372. Acta Oncol. 2004. PMID: 15360046 Review.
-
Reflectance confocal microscopy for the diagnosis of vulvar melanoma and melanosis: preliminary results.Dermatol Surg. 2012 Dec;38(12):1962-7. doi: 10.1111/dsu.12009. Epub 2012 Nov 5. Dermatol Surg. 2012. PMID: 23127153
Cited by
-
Robot-assisted laparoscopic hepatectomy for liver metastasis from clitoral malignant melanoma: a case report.Surg Case Rep. 2024 Nov 11;10(1):258. doi: 10.1186/s40792-024-02058-7. Surg Case Rep. 2024. PMID: 39527378 Free PMC article.
-
Genitourinary melanoma: An overview for the clinician.Asian J Urol. 2022 Oct;9(4):407-422. doi: 10.1016/j.ajur.2022.01.003. Epub 2022 Jun 2. Asian J Urol. 2022. PMID: 36381597 Free PMC article. Review.
-
Clitoral metastasis of vulvar melanoma treated with talimogene laherparepvec.JAAD Case Rep. 2022 Dec 5;32:15-17. doi: 10.1016/j.jdcr.2022.11.032. eCollection 2023 Feb. JAAD Case Rep. 2022. PMID: 36620496 Free PMC article. No abstract available.
-
Pancreatic Metastasis From a Vulvar Melanoma Diagnosed by Endoscopic Ultrasound-Guided Fine-Needle Biopsy.ACG Case Rep J. 2025 Aug 21;12(8):e01784. doi: 10.14309/crj.0000000000001784. eCollection 2025 Aug. ACG Case Rep J. 2025. PMID: 40851797 Free PMC article.
-
Female patient perspective on the incorporation of genital skin examination during routine total body skin exams.Arch Dermatol Res. 2024 Jan 23;316(2):80. doi: 10.1007/s00403-024-02821-8. Arch Dermatol Res. 2024. PMID: 38263480 No abstract available.
References
-
- Ragnarsson-Olding B, Johansson H, Rutqvist LE, Ringborg U. Malignant melanoma of the vulva and vagina: trends in incidence, age distribution, and long-term survival among 245 consecutive cases in Sweden 1960–1984. Cancer. 1993;71:1893–1897. doi: 10.1002/1097-0142(19930301)71:5<1893::AID-CNCR2820710528>3.0.CO;2-7. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
