

Detection of myocardial ischemia by intracoronary ECG using convolutional neural networks
- PMID: 34125855
- PMCID: PMC8202932
- DOI: 10.1371/journal.pone.0253200
Detection of myocardial ischemia by intracoronary ECG using convolutional neural networks
Abstract
Introduction: The electrocardiogram (ECG) is a valuable tool for the diagnosis of myocardial ischemia as it presents distinctive ischemic patterns. Deep learning methods such as convolutional neural networks (CNN) are employed to extract data-derived features and to recognize natural patterns. Hence, CNN enable an unbiased view on well-known clinical phenomenon, e.g., myocardial ischemia. This study tested a novel, hypothesis-generating approach using pre-trained CNN to determine the optimal ischemic parameter as obtained from the highly susceptible intracoronary ECG (icECG).
Method: This was a retrospective observational study in 228 patients with chronic coronary syndrome. Each patient had participated in clinical trials with icECG recording and ST-segment shift measurement at the beginning (i.e., non-ischemic) and the end (i.e., ischemic) of a one-minute proximal coronary artery balloon occlusion establishing the reference. Using these data (893 icECGs in total), two pre-trained, open-access CNN (GoogLeNet/ResNet101) were trained to recognize ischemia. The best performing CNN during training were compared with the icECG ST-segment shift for diagnostic accuracy in the detection of artificially induced myocardial ischemia.
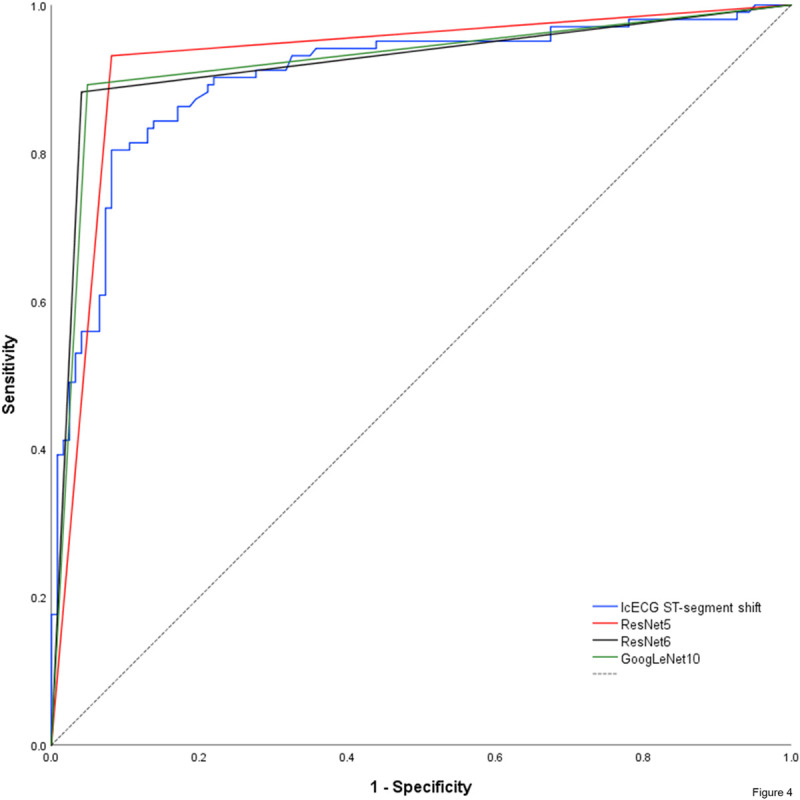
Results: Using coronary patency or occlusion as reference for absent or present myocardial ischemia, receiver-operating-characteristics (ROC)-analysis of manually obtained icECG ST-segment shift (mV) showed an area under the ROC-curve (AUC) of 0.903±0.043 (p<0.0001, sensitivity 80%, specificity 92% at a cut-off of 0.279mV). The best performing CNN showed an AUC of 0.924 (sensitivity 93%, specificity 92%). DeLong-Test of the ROC-curves showed no significant difference between the AUCs. The underlying morphology responsible for the network prediction differed between the trained networks but was focused on the ST-segment and the T-wave for myocardial ischemia detection.
Conclusions: When tested in an experimental setting with artificially induced coronary artery occlusion, quantitative icECG ST-segment shift and CNN using pathophysiologic prediction criteria detect myocardial ischemia with similarly high accuracy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Accuracy of intracoronary ECG parameters for myocardial ischemia detection.J Electrocardiol. 2021 Jan-Feb;64:50-57. doi: 10.1016/j.jelectrocard.2020.11.018. Epub 2020 Dec 5. J Electrocardiol. 2021. PMID: 33316551
-
Intracoronary ECG ST-segment shift remission time during reactive myocardial hyperemia: a new method to assess hemodynamic coronary stenosis severity.Am J Physiol Heart Circ Physiol. 2024 Oct 1;327(4):H1124-H1131. doi: 10.1152/ajpheart.00481.2024. Epub 2024 Sep 6. Am J Physiol Heart Circ Physiol. 2024. PMID: 39240257 Free PMC article.
-
Algorithm for real-time analysis of intracoronary electrocardiogram.Front Cardiovasc Med. 2022 Sep 7;9:930717. doi: 10.3389/fcvm.2022.930717. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36172580 Free PMC article.
-
Electrocardiographic ST-segment changes during acute myocardial ischemia.Card Electrophysiol Rev. 2002 Sep;6(3):196-203. doi: 10.1023/a:1016352205286. Card Electrophysiol Rev. 2002. PMID: 12114838 Review.
-
Context-independent identification of myocardial ischemia in the prehospital ECG of chest pain patients.J Electrocardiol. 2024 Jan-Feb;82:34-41. doi: 10.1016/j.jelectrocard.2023.10.009. Epub 2023 Nov 7. J Electrocardiol. 2024. PMID: 38006762 Review.
Cited by
-
Prognostic and diagnostic accuracy of intracoronary electrocardiogram recorded during percutaneous coronary intervention: a meta-analysis.BMJ Open. 2022 Jun 29;12(6):e055871. doi: 10.1136/bmjopen-2021-055871. BMJ Open. 2022. PMID: 35768115 Free PMC article.
-
Meta-Analysis of Dynamic Electrocardiography in the Diagnosis of Myocardial Ischemic Attack of Coronary Heart Disease.Comput Math Methods Med. 2022 Jun 7;2022:3472413. doi: 10.1155/2022/3472413. eCollection 2022. Comput Math Methods Med. 2022. Retraction in: Comput Math Methods Med. 2023 Jun 28;2023:9838452. doi: 10.1155/2023/9838452. PMID: 35712003 Free PMC article. Retracted.
-
Deep learning and electrocardiography: systematic review of current techniques in cardiovascular disease diagnosis and management.Biomed Eng Online. 2025 Feb 23;24(1):23. doi: 10.1186/s12938-025-01349-w. Biomed Eng Online. 2025. PMID: 39988715 Free PMC article.
-
Primary versus iatrogenic (post-PCI) coronary microvascular dysfunction: a wire-based multimodal comparison.Open Heart. 2023 Nov 27;10(2):e002437. doi: 10.1136/openhrt-2023-002437. Open Heart. 2023. PMID: 38011991 Free PMC article. Clinical Trial.
-
State-of-the-Art Deep Learning Methods on Electrocardiogram Data: Systematic Review.JMIR Med Inform. 2022 Aug 15;10(8):e38454. doi: 10.2196/38454. JMIR Med Inform. 2022. PMID: 35969441 Free PMC article. Review.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al.. (2018) 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC), Eur Heart J.39 119–177 doi: 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Goodfellow I, Bengio Y, Courville A (2016) Deep Learning MIT Press.
