

Endovascular thrombectomy and intra-arterial interventions for acute ischaemic stroke
- PMID: 34125952
- PMCID: PMC8203212
- DOI: 10.1002/14651858.CD007574.pub3
Endovascular thrombectomy and intra-arterial interventions for acute ischaemic stroke
Abstract
Background: Most disabling strokes are due to a blockage of a large artery in the brain by a blood clot. Prompt removal of the clot with intra-arterial thrombolytic drugs or mechanical devices, or both, can restore blood flow before major brain damage has occurred, leading to improved recovery. However, these so-called endovascular interventions can cause bleeding in the brain. This is a review of randomised controlled trials of endovascular thrombectomy or intra-arterial thrombolysis, or both, for acute ischaemic stroke.
Objectives: To assess whether endovascular thrombectomy or intra-arterial interventions, or both, plus medical treatment are superior to medical treatment alone in people with acute ischaemic stroke.
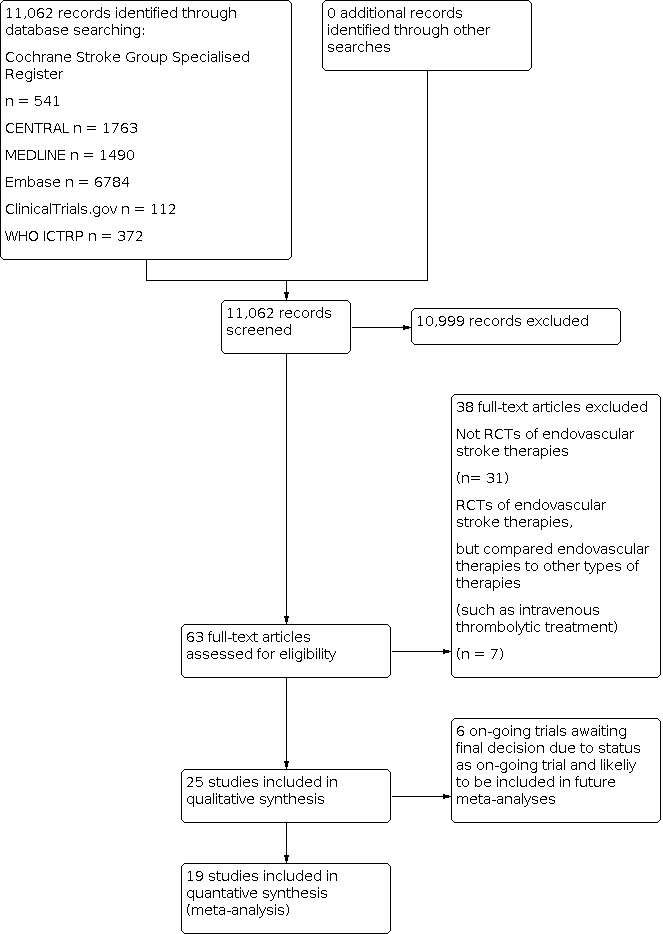
Search methods: We searched the Trials Registers of the Cochrane Stroke Group and Cochrane Vascular Group (last searched 1 September 2020), CENTRAL (the Cochrane Library, 1 September 2020), MEDLINE (May 2010 to 1 September 2020), and Embase (May 2010 to 1 September 2020). We also searched trials registers, screened reference lists, and contacted researchers.
Selection criteria: Randomised controlled trials (RCTs) of any endovascular intervention plus medical treatment compared with medical treatment alone in people with definite ischaemic stroke.
Data collection and analysis: Two review authors (MBR and MJ) applied the inclusion criteria, extracted data, and assessed trial quality. Two review authors (MBR and HL) assessed risk of bias, and the certainty of the evidence using GRADE. We obtained both published and unpublished data if available. Our primary outcome was favourable functional outcome at the end of the scheduled follow-up period, defined as a modified Rankin Scale score of 0 to 2. Eighteen trials (i.e. all but one included trial) reported their outcome at 90 days. Secondary outcomes were death from all causes at in the acute phase and by the end of follow-up, symptomatic intracranial haemorrhage in the acute phase and by the end of follow-up, neurological status at the end of follow-up, and degree of recanalisation.
Main results: We included 19 studies with a total of 3793 participants. The majority of participants had large artery occlusion in the anterior circulation, and were treated within six hours of symptom onset with endovascular thrombectomy. Treatment increased the chance of achieving a good functional outcome, defined as a modified Rankin Scale score of 0 to 2: risk ratio (RR) 1.50 (95% confidence interval (CI) 1.37 to 1.63; 3715 participants, 18 RCTs; high-certainty evidence). Treatment also reduced the risk of death at end of follow-up: RR 0.85 (95% CI 0.75 to 0.97; 3793 participants, 19 RCTs; high-certainty evidence) without increasing the risk of symptomatic intracranial haemorrhage in the acute phase: RR 1.46 (95% CI 0.91 to 2.36; 1559 participants, 6 RCTs; high-certainty evidence) or by end of follow-up: RR 1.05 (95% CI 0.72 to 1.52; 1752 participants, 10 RCTs; high-certainty evidence); however, the wide confidence intervals preclude any firm conclusion. Neurological recovery to National Institutes of Health Stroke Scale (NIHSS) score 0 to 1 and degree of recanalisation rates were better in the treatment group: RR 2.03 (95% CI 1.21 to 3.40; 334 participants, 3 RCTs; high-certainty evidence) and RR 3.11 (95% CI 2.18 to 4.42; 268 participants, 3 RCTs; high-certainty evidence), respectively.
Authors' conclusions: In individuals with acute ischaemic stroke due to large artery occlusion in the anterior circulation, endovascular thrombectomy can increase the chance of survival with a good functional outcome without increasing the risk of intracerebral haemorrhage or death.
Trial registration: ClinicalTrials.gov NCT01717755 NCT01852201 NCT02419781 NCT03094715 NCT03805308.
Copyright © 2021 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
Melinda B Roaldsen:
Grants and contracts: National Institute for Health Research (NIHR) Cochrane Review Incentive Scheme to be paid on publication of this update. The award will be received by my institution.
Work as a health professional: "I am a MD and hold a position as a Resident at the Neurological Department in Tromsø, Norway. Currently on leave from clinical work to do research."
Institution: University Hospital of North Norway, Tromsø, Norway
Mirza Jusufovic: none known Eivind Berge: none known (deceased) Haakon Lindekleiv: none known
Figures























Update of
-
Percutaneous vascular interventions for acute ischaemic stroke.Cochrane Database Syst Rev. 2010 Oct 6;(10):CD007574. doi: 10.1002/14651858.CD007574.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2021 Jun 14;6:CD007574. doi: 10.1002/14651858.CD007574.pub3. PMID: 20927761 Updated.
References
References to studies included in this review
AUST 2005 {published and unpublished data}
-
- Macleod M, Davis S, Mitchell P, Gerraty RP, Fitt G, Hankey GJ, et al.Results of a multicentre, randomised controlled trial of intra-arterial urokinase in the treatment of acute posterior circulation ischaemic stroke. Cerebrovascular Diseases 2005;20:12-7. - PubMed
BEST 2019 {published data only}
-
- Liu X, Dai Q, Ye R, Zi W, Liu Y, Wang H, et al.Endovascular treatment versus standard medical treatment for vertebrobasilar artery occlusion (BEST): an open-label, randomised controlled trial. Lancet Neurology 2020;19:115-22. - PubMed
DAWN 2018 {published data only}
-
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al.Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. New England Journal of Medicine 2018;378:11-21. - PubMed
DEFUSE 2018 {published data only}
EASI 2017 {published data only}
-
- Khoury NN, Darsaut TE, Ghostine J, Deschaintre Y, Daneault N, Durocher A, et al.Endovascular thrombectomy and medical therapy versus medical therapy alone in acute stroke: a randomised care trial. Journal of Neuroradiology 2017;44(3):198-202. - PubMed
ESCAPE 2015 {published data only}
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al.Randomized assessment of rapid endovascular treatment of ischemic stroke. New England Journal of Medicine 2015;372:1019-30. - PubMed
EXTEND‐IA 2015 {published data only}
-
- Campbell BCV, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al.Endovascular therapy for ischemic stroke with perfusion-imaging selection. New England Journal of Medicine 2015;372:1009-18. - PubMed
IMS III 2013 {published data only}
MELT 2007 {published and unpublished data}
-
- Ogawa A, Mori E, Minematsu K, Taki W, Takahashi A, Nemoto S, et al.Randomised trial of intra-arterial infusion of urokinase within 6 hours of middle cerebral artery stroke. Stroke 2007;38:2633-9. - PubMed
MR CLEAN 2015 {published data only}
-
- Berkhemer OA, Fransen PSS, Beumer D, den Berg LA, Lingsma HF, Yoo AJ, et al.A randomized trial of intraarterial treatment for acute ischemic stroke. New England Journal of Medicine 2015;371:11-20. - PubMed
MR RESCUE 2013 {published data only}
PISTE 2016 {published data only}
PROACT 1 1998 {published data only (unpublished sought but not used)}
-
- Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA, Gent M, et al.PROACT: a phase II trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. Stroke 1998;29:4-11. - PubMed
PROACT 2 1999 {published data only (unpublished sought but not used)}
-
- Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al.Intra-arterial pro-urokinase for acute ischaemic stroke: the PROACT II study: a randomised controlled trial. JAMA 1999;282:2003-11. - PubMed
RESILIENT 2020 {published data only}
-
- Martins SO, Mont’Alverne F, Rebello LC, Abud DG, Silva GS, Lima FO, et al.Thrombectomy for stroke in the public health care system of Brazil. New England Journal of Medicine 2020;382:2316-26. [ClinicalTrials.gov: NCT02216643] - PubMed
REVASCAT 2015 {published data only}
-
- Jovin TG, Chamorro A, Cobo E, Miquel MA, Molina CA, Rovira A, et al.Thrombectomy within 8 hours after symptom onset in ischemic stroke. New England Journal of Medicine 2015;372:2296-306. - PubMed
SWIFT PRIME 2015 {published data only}
-
- Saver JL, Goyal M, Bonafe A, Diener H-C, Levy EI, Pereira VM, et al.Stent-retriever thrombectomy after intravenous t-PA vs t-PA alone in stroke. New England Journal of Medicine 2015;372:2285-95. - PubMed
THERAPY 2016 {published data only}
-
- Mocco J, Zaidat OO, Kummer R, Yoo AJ, Gupta R, Lopes D, et al.Aspiration thrombectomy after intravenous alteplase versus intravenous alteplase alone. Stroke 2016;47:2331-8. - PubMed
THRACE 2016 {published data only}
-
- Bracard S, Ducrocq X, Mas JL, Soudant M, Oppenheim C, Moulin T, et al.Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurology 2016;15:1138-47. - PubMed
References to studies excluded from this review
Ducrocq 2005 {published data only}
-
- Ducrocq X, Bracard S, Taillandier L, Anxionnat R, Lacour JC, Guillemin F, et al.Comparison of intravenous and intra-arterial urokinase thrombolysis for acute ischaemic stroke. Journal of Neuroradiology 2005;32:26-32. - PubMed
Keris 2001 {published data only}
Lewandowski 1999 {published data only}
-
- Lewandowski CA, Frankel M, Tomsick TA, Broderick J, Frey J, Clark W, et al.Combined intravenous and intra-arterial r-TPA versus intra-arterial therapy of acute ischemic stroke: Emergency Management of Stroke (EMS) Bridging Trial. Stroke 1999;30:2598-605. - PubMed
Sen 2009 {published data only}
-
- Sen S, Huang DY, Akhavan O, Wilson S, Verro P, Solander S, et al.IV vs IA TPA in acute ischemic stroke with CT angiographic evidence of major vessel occlusion: a feasibility study. Neurocritical Care 2009;11:76-81. - PubMed
SYNTHESIS Expansion 2013 {published data only}
SYNTHESIS pilot 2010 {published data only}
-
- Ciccone A, Valvassori L, Ponzio M, Ballabio M, Gasparotti R, Sessa M, et al.Intra‐arterial or intravenous thrombolysis for acute ischemic stroke? The SYNTHESIS pilot trial. Journal of Neurointerventional Surgery 2010;2:74‐9. - PubMed
Wolfe 2008 {published data only}
-
- Wolfe T, Suarez JI, Tarr RW, Welter E, Landis D, Sunshine JL, et al.Comparison of combined venous and arterial thrombolysis with primary arterial therapy using recombinant tissue plasminogen activator in acute ischemic stroke. Journal of Stroke and Cerebrovascular Diseases 2008;17:121-8. - PubMed
References to ongoing studies
ISRCTN19922220 {published data only}ISRCTN19922220
-
- ISRCTN19922220.Endovascular treatment of acute ischemic stroke in the Netherlands for late arrivals. www.isrctn.com/ISRCTN19922220 (first received 11 December 2017). [DOI: 10.1186/ISRCTN19922220] - DOI
NCT01717755 {published data only}
-
- NCT01717755.Basilar Artery International Cooperation Study (BASICS). clinicaltrials.gov/ct2/show/NCT01717755 (first received 30 October 2012).
NCT01852201 {published data only}
-
- NCT01852201.POSITIVE Stroke Clinical Trial. clinicaltrials.gov/ct2/show/NCT01852201 (first received 13 May 2013).
NCT02419781 {published data only}
-
- NCT02419781.Recovery by Endovascular Salvage for Cerebral Ultra-acute Embolism (RESCUE)-Japan RCT. clinicaltrials.gov/ct2/show/NCT02419781 (first received 17 April 2015).
NCT03094715 {published data only}
-
- NCT03094715.Efficacy and safety of thrombectomy in stroke with extended lesion and extended time window (TENSION). clinicaltrials.gov/ct2/show/NCT03094715 (first received 29 March 2017).
NCT03805308 {published data only}
-
- NCT03805308.The TESLA Trial: Thrombectomy for Emergent Salvage of Large Anterior circulation ischemic stroke (TESLA). clinicaltrials.gov/ct2/show/NCT03805308 (first received 15 January 2019).
Additional references
Deeks 2001
-
- Deeks JJ, Altman DG, Bradburn MJ.Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Davey Smith G, Altman DG, editors(s). Systematic Reviews in Health Care: Meta-analysis in Context. 2nd edition. London: BMJ Publication Group, 2001.
GRADE Pro GDT 2020 [Computer program]
-
- GRADEpro GDT: GRADEpro Guideline Development Tool [Software].Available from gradepro.org, McMaster University, 2020 (developed by Evidence Prime, Inc.).
Hacke 1995
-
- Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, Kummer R, et al.Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS). JAMA 1995;274:1017-25. - PubMed
Higashida 2003
-
- Higashida R, Furlan A.Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke 2003;34:e109-37. - PubMed
Higgins 2011
-
- Higgins JPT, Green S editor(s).Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0 (updated March 2011). Cochrane, 2011. Available from www.handbook.cochrane.org.
Higgins 2021
-
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s).Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021). Cochrane, 2021. Available from www.training.cochrane.org/handbook.
Khatri 2005
-
- Khatri P, Neff J, Broderick J, Khoury JC, Carrozzella J, Tomsick T.Revascularization end points in stroke interventional trials: recanalization versus reperfusion in IMS-I. Stroke 2005;36:2400-3. - PubMed
Lin 2019
NINDS 1995
-
- The NINDS rt-PA Stroke Study Group.Tissue plasminogen activator for acute ischemic stroke. New England Journal of Medicine 1995;333:1581-7. - PubMed
Nogueira 2013
-
- Nogueira R, Gupta R, Davalos A.IMS-III and SYNTHESIS expansion trials of endovascular therapy in acute ischaemic stroke. Stroke 2013;44:3272-4. - PubMed
Review Manager 2020 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration Review Manager (RevMan).Version 5.4. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2020.
Saver 2007
-
- Saver J.Intra-arterial fibrinolysis for acute ischaemic stroke. The message of Melt. Stroke 2007;38:2627-8. - PubMed
Wardlaw 2009
Warlow 2003
-
- Warlow C, Sudlow C, Dennis M, Sandercock P.Stroke. Lancet 2003;362:1211-24. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical