

Discontinuation versus continuation of renin-angiotensin-system inhibitors in COVID-19 (ACEI-COVID): a prospective, parallel group, randomised, controlled, open-label trial
- PMID: 34126053
- PMCID: PMC8195495
- DOI: 10.1016/S2213-2600(21)00214-9
Discontinuation versus continuation of renin-angiotensin-system inhibitors in COVID-19 (ACEI-COVID): a prospective, parallel group, randomised, controlled, open-label trial
Erratum in
-
Correction to Lancet Respir Med 2021; published online June 11. https://doi.org/10.1016/S2213-2600(21)00214-9.Lancet Respir Med. 2021 Sep;9(9):e95. doi: 10.1016/S2213-2600(21)00362-3. Epub 2021 Aug 6. Lancet Respir Med. 2021. PMID: 34370975 Free PMC article. No abstract available.
Abstract
Background: SARS-CoV-2 entry in human cells depends on angiotensin-converting enzyme 2, which can be upregulated by inhibitors of the renin-angiotensin system (RAS). We aimed to test our hypothesis that discontinuation of chronic treatment with ACE-inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) mitigates the course o\f recent-onset COVID-19.
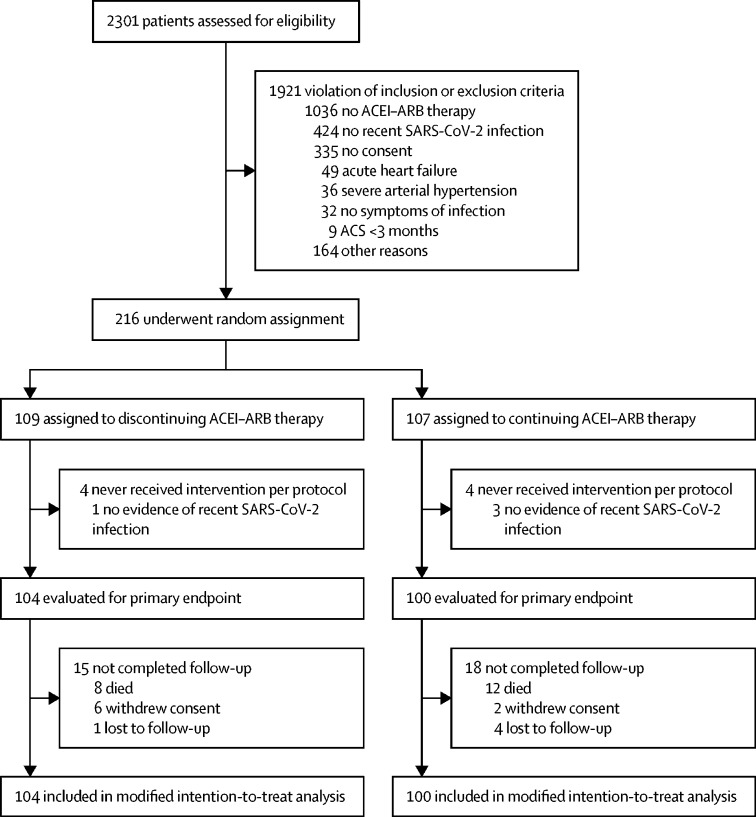
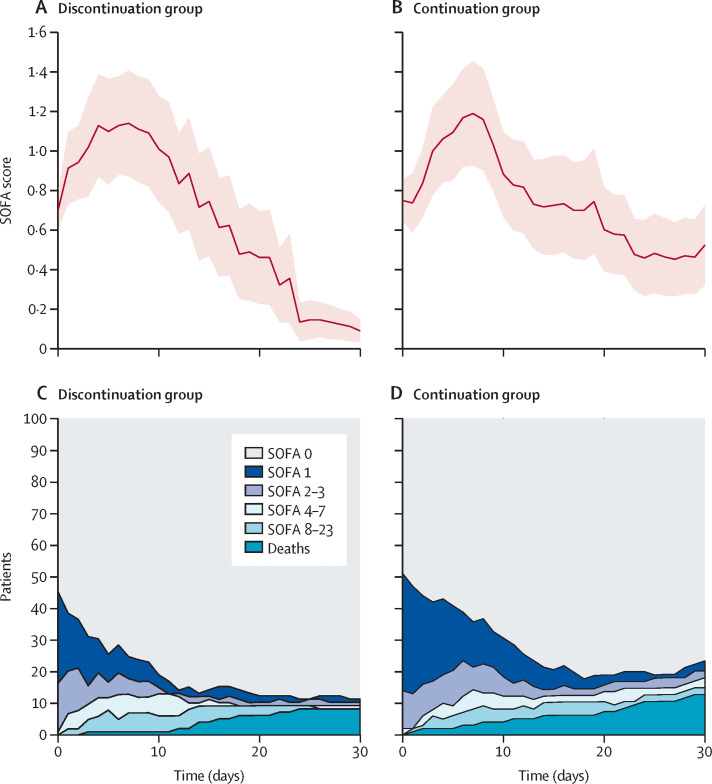
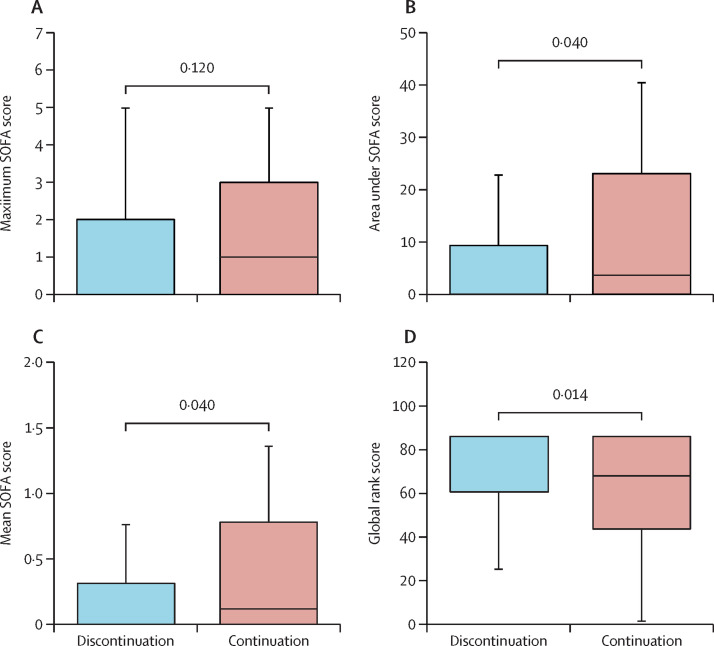
Methods: ACEI-COVID was a parallel group, randomised, controlled, open-label trial done at 35 centres in Austria and Germany. Patients aged 18 years and older were enrolled if they presented with recent symptomatic SARS-CoV-2 infection and were chronically treated with ACEIs or ARBs. Patients were randomly assigned 1:1 to discontinuation or continuation of RAS inhibition for 30 days. Primary outcome was the maximum sequential organ failure assessment (SOFA) score within 30 days, where death was scored with the maximum achievable SOFA score. Secondary endpoints were area under the death-adjusted SOFA score (AUCSOFA), mean SOFA score, admission to the intensive care unit, mechanical ventilation, and death. Analyses were done on a modified intention-to-treat basis. This trial is registered with ClinicalTrials.gov, NCT04353596.
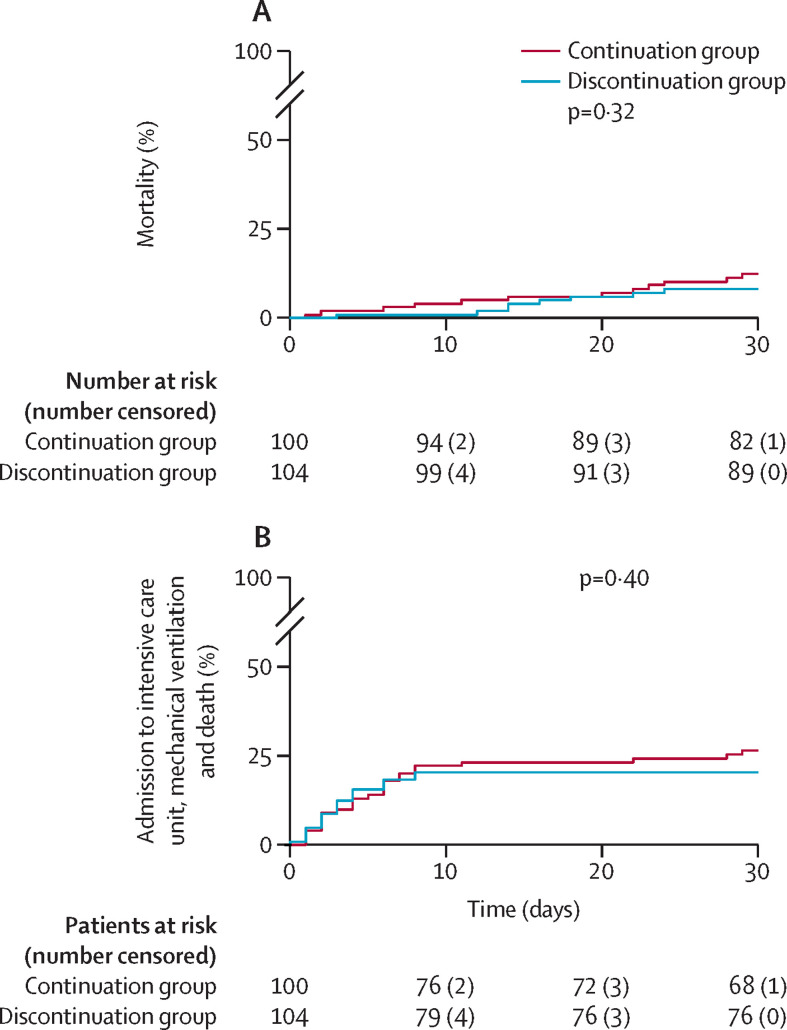
Findings: Between April 20, 2020, and Jan 20, 2021, 204 patients (median age 75 years [IQR 66-80], 37% females) were randomly assigned to discontinue (n=104) or continue (n=100) RAS inhibition. Within 30 days, eight (8%) of 104 died in the discontinuation group and 12 (12%) of 100 patients died in the continuation group (p=0·42). There was no significant difference in the primary endpoint between the discontinuation and continuation group (median [IQR] maximum SOFA score 0·00 (0·00-2·00) vs 1·00 (0·00-3·00); p=0·12). Discontinuation was associated with a significantly lower AUCSOFA (0·00 [0·00-9·25] vs 3·50 [0·00-23·50]; p=0·040), mean SOFA score (0·00 [0·00-0·31] vs 0·12 [0·00-0·78]; p=0·040), and 30-day SOFA score (0·00 [10-90th percentile, 0·00-1·20] vs 0·00 [0·00-24·00]; p=0·023). At 30 days, 11 (11%) in the discontinuation group and 23 (23%) in the continuation group had signs of organ dysfunction (SOFA score ≥1) or were dead (p=0·017). There were no significant differences for mechanical ventilation (10 (10%) vs 8 (8%), p=0·87) and admission to intensive care unit (20 [19%] vs 18 [18%], p=0·96) between the discontinuation and continuation group.
Interpretation: Discontinuation of RAS-inhibition in COVID-19 had no significant effect on the maximum severity of COVID-19 but may lead to a faster and better recovery. The decision to continue or discontinue should be made on an individual basis, considering the risk profile, the indication for RAS inhibition, and the availability of alternative therapies and outpatient monitoring options.
Funding: Austrian Science Fund and German Center for Cardiovascular Research.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests AB received research funding from Pfizer and Medtronic as well as speaker honoraria from Bayer, Boehringer Ingelheim, Edwards, Medtronic and Novartis. KDR received a research grant from Daiichi-Sankyo Europe GmbH. UM received fees for participation in a data and safety monitoring board from Thermosome. All other authors declare no competing interests.
Figures
References
-
- John Hopkins Coronavirus Resource Center COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. 2021. https://coronavirus.jhu.edu/map.html
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239–1242. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
