

Evidence-Based Management of Hepatocellular Carcinoma: Systematic Review and Meta-analysis of Randomized Controlled Trials (2002-2020)
- PMID: 34126063
- PMCID: PMC12276942
- DOI: 10.1053/j.gastro.2021.06.008
Evidence-Based Management of Hepatocellular Carcinoma: Systematic Review and Meta-analysis of Randomized Controlled Trials (2002-2020)
Abstract
Background & aims: Hepatocellular carcinoma (HCC) is a leading cause of cancer-related mortality, with a rapidly changing landscape of treatments. In the past 20 years, numerous randomized controlled trials (RCTs) have aimed at improving outcomes across disease stages. We aimed to analyze the current evidence and identify potential factors influencing response to therapies.
Methods: We conducted a systematic review of phase III RCTs (2002-2020) across disease stages. A meta-analysis was designed to examine the relationship between etiology and outcome after systemic therapies with either tyrosine-kinase inhibitor (TKI)/antiangiogenic or immune checkpoint inhibitor (ICI) therapy.
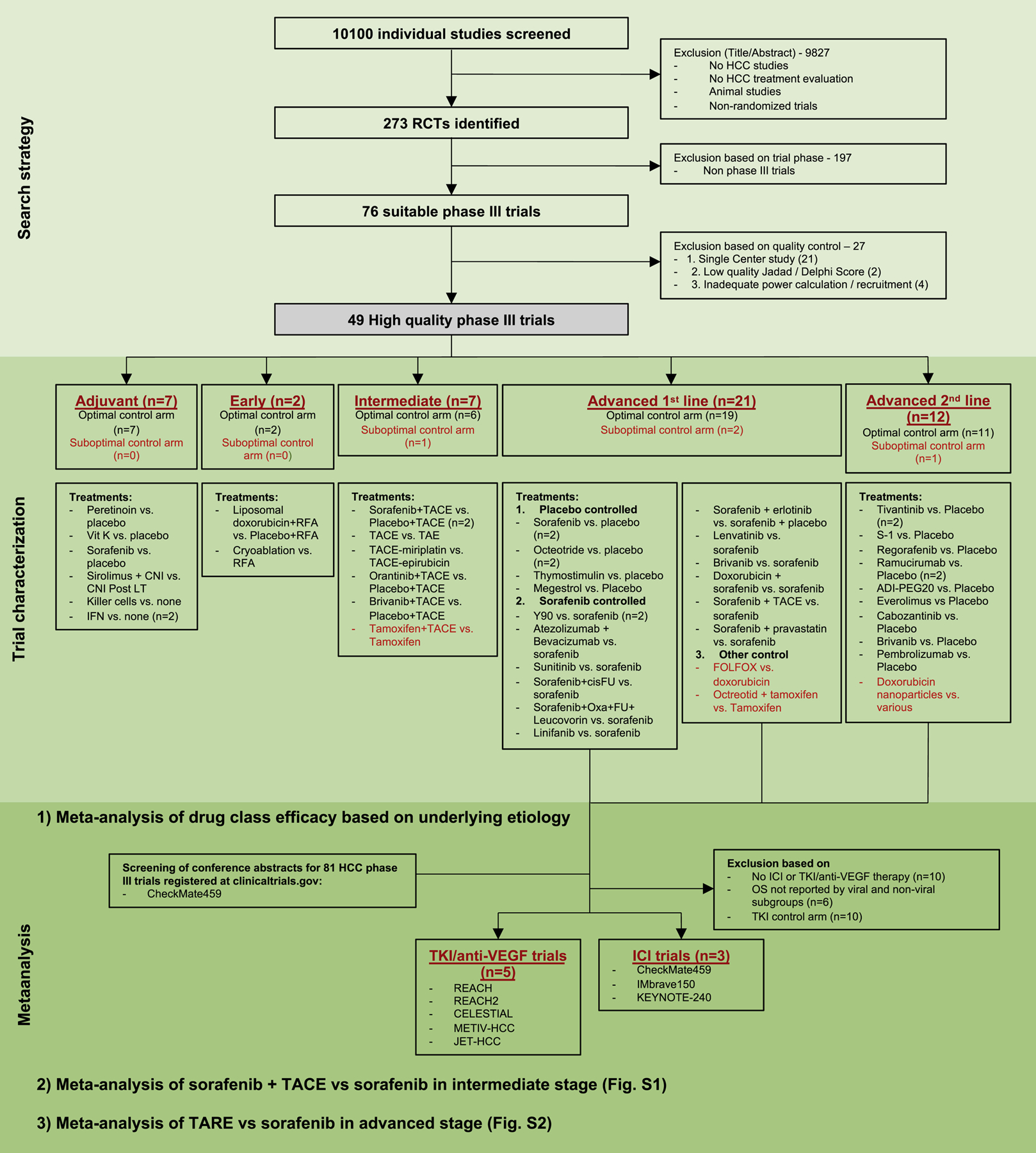
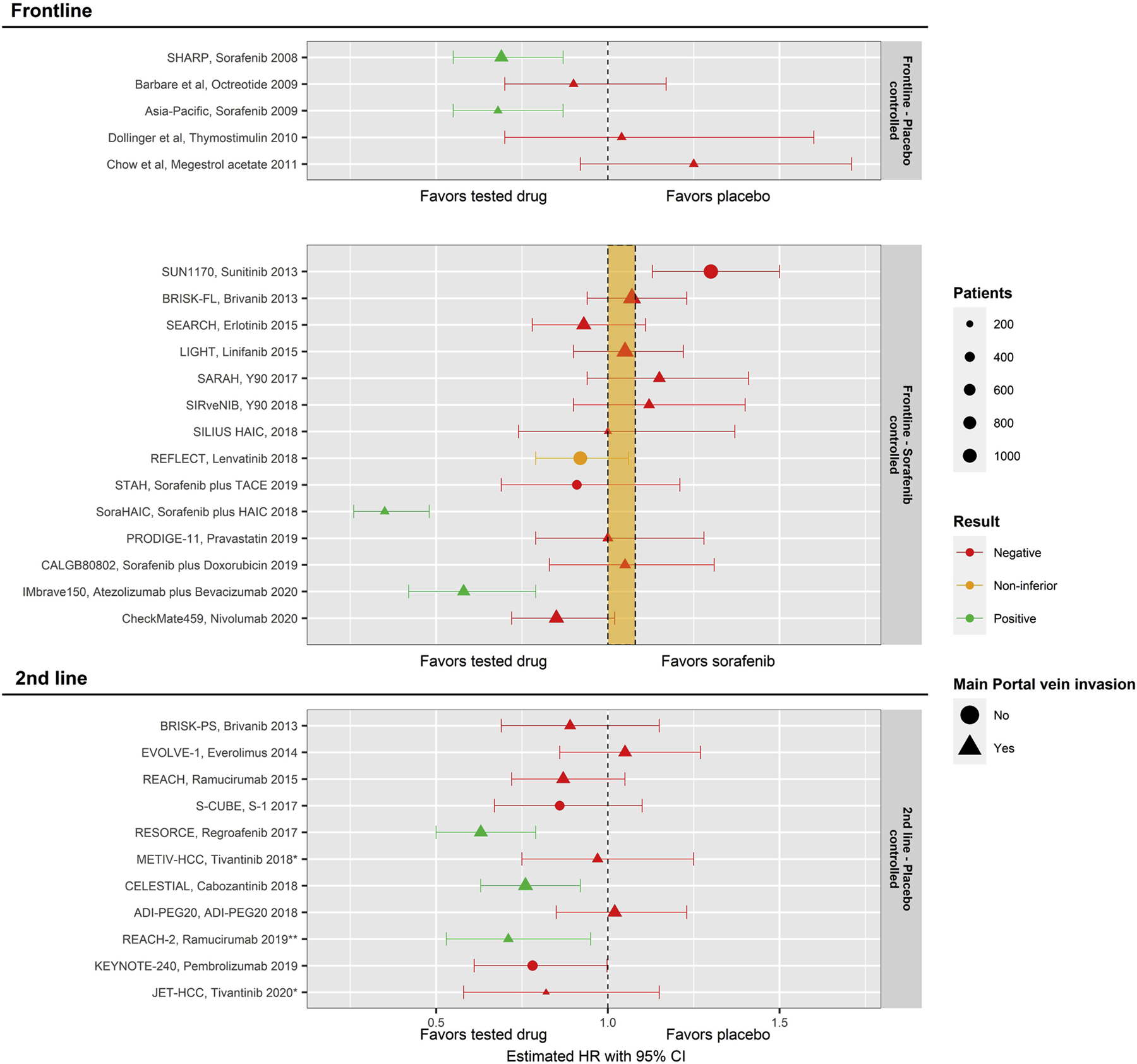
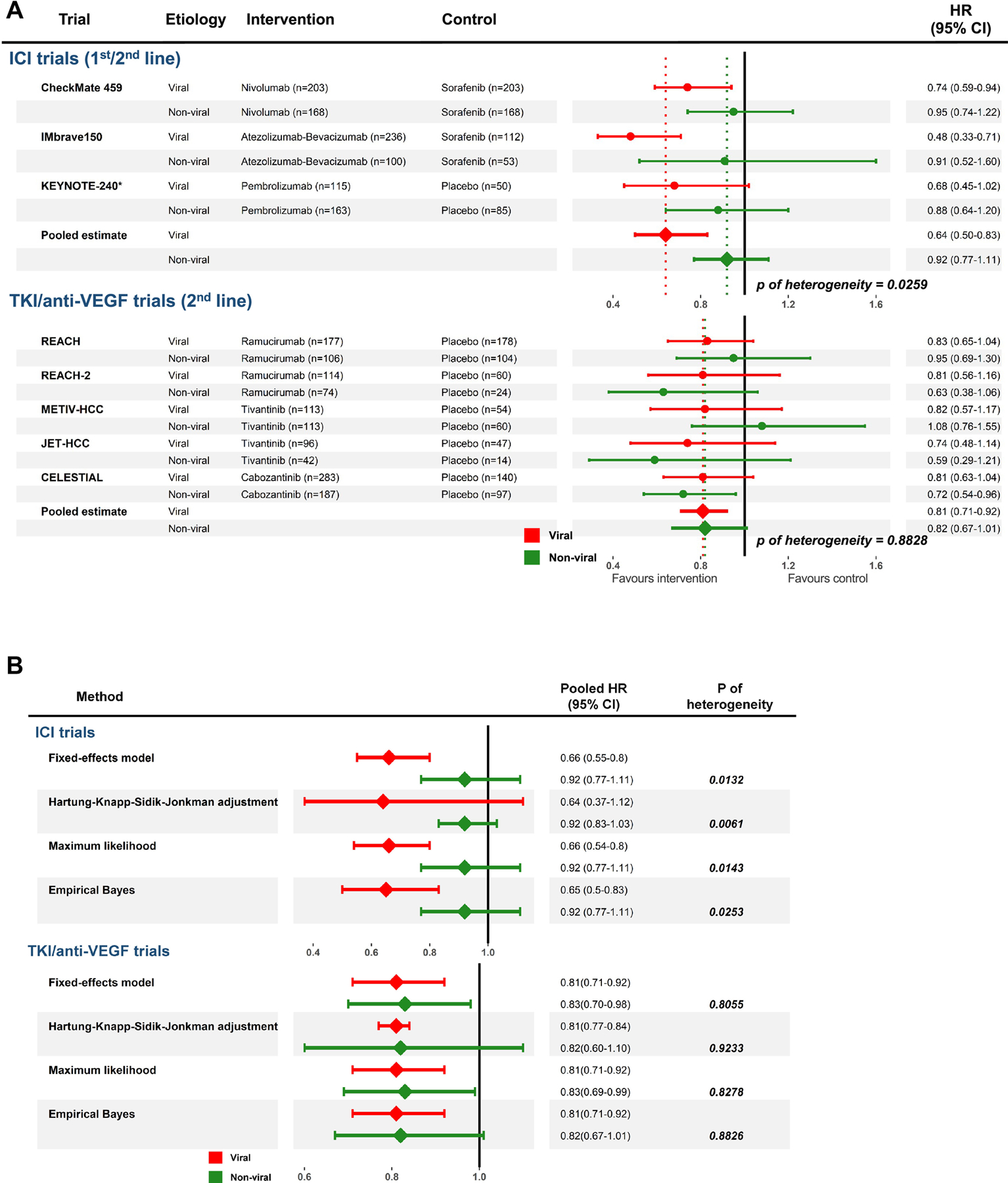
Results: Out of 10,100 studies identified, 76 were phase III RCTs. Among them, a rigorous screening algorithm identified 49 with high quality including a total of 22,113 patients undergoing adjuvant (n = 7) and primary treatment for early (n = 2), intermediate (n = 7), and advanced (first-line, n = 21; second-line, n = 12) stages of disease. Nine of these trials were positive, 6 treatments have been adopted in guidelines (sorafenib [2 RCTs], lenvatinib, atezolizumab+bevacizumab, regorafenib, cabozantinib and ramucirumab), but 2 were not (adjuvant CIK cells and sorafenib plus hepatic arterial infusion with FOLFOX). Meta-analysis of 8 trials including 3739 patients revealed ICI therapy to be significantly more effective in patients with viral hepatitis compared with nonviral-related HCC, whereas no differences related to etiology were observed in patients treated with TKI/anti-vascular endothelial growth factor.
Conclusions: Among 49 high-quality RCTs conducted in HCC during 2002-2020, 9 resulted in positive results. A meta-analysis of systemic therapies suggests that immunotherapies may be more effective in viral etiologies.
Keywords: Hepatocellular carcinoma; Liver cancer; Randomized controlled trials; Systematic review.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
R.M. has received lecture or consulting fees from Roche and Servier. A.V. has received consulting fees from Guidepoint, Fujifilm, Boehringer Ingelheim, FirstWord, and MHLife. J.M.L. is receiving research support from Bayer HealthCare Pharmaceuticals, Eisai, Bristol-Myers Squibb, Boehringer-Ingelheim, and Ipsen, and consulting fees from Eli Lilly, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb, Eisai, Celsion Corporation, Exelixis, Merck, Ipsen, Genentech, Roche, Glycotest, Nucleix, Sirtex, Mina Alpha, and AstraZeneca. The other authors declare no conflicts.
Figures
Comment in
-
Viral Etiology of Solid Tumors and Immunotherapy.Gastroenterology. 2022 Feb;162(2):659-660. doi: 10.1053/j.gastro.2021.09.048. Epub 2021 Sep 25. Gastroenterology. 2022. PMID: 34582894 No abstract available.
Similar articles
-
Sequencing of systemic therapy in unresectable hepatocellular carcinoma: A systematic review and Bayesian network meta-analysis of randomized clinical trials.Crit Rev Oncol Hematol. 2024 Dec;204:104522. doi: 10.1016/j.critrevonc.2024.104522. Epub 2024 Sep 26. Crit Rev Oncol Hematol. 2024. PMID: 39332750
-
Systemic Therapy and Sequencing Options in Advanced Hepatocellular Carcinoma: A Systematic Review and Network Meta-analysis.JAMA Oncol. 2020 Dec 1;6(12):e204930. doi: 10.1001/jamaoncol.2020.4930. Epub 2020 Dec 10. JAMA Oncol. 2020. PMID: 33090186 Free PMC article.
-
Management of people with early- or very early-stage hepatocellular carcinoma: an attempted network meta-analysis.Cochrane Database Syst Rev. 2017 Mar 28;3(3):CD011650. doi: 10.1002/14651858.CD011650.pub2. Cochrane Database Syst Rev. 2017. PMID: 28351116 Free PMC article.
-
Efficacy and safety of first-line treatments for advanced hepatocellular carcinoma patients: a systematic review and network meta-analysis.Front Immunol. 2024 Sep 17;15:1430196. doi: 10.3389/fimmu.2024.1430196. eCollection 2024. Front Immunol. 2024. PMID: 39355238 Free PMC article.
-
Ablative and non-surgical therapies for early and very early hepatocellular carcinoma: a systematic review and network meta-analysis.Health Technol Assess. 2023 Dec;27(29):1-172. doi: 10.3310/GK5221. Health Technol Assess. 2023. PMID: 38149643 Free PMC article.
Cited by
-
Efficacy and safety of regorafenib as second-line treatment for patients with hepatocellular carcinoma and macrovascular invasion and(or) extrahepatic metastasis.J Gastrointest Oncol. 2023 Dec 31;14(6):2536-2548. doi: 10.21037/jgo-23-651. Epub 2023 Nov 21. J Gastrointest Oncol. 2023. PMID: 38196538 Free PMC article.
-
Efficacy and safety of PD-1 inhibitors plus anti-angiogenesis tyrosine kinase inhibitors with or without transarterial chemo(embolization) for unresectable hepatocellular carcinoma: a meta-analysis.Front Oncol. 2024 Aug 22;14:1364345. doi: 10.3389/fonc.2024.1364345. eCollection 2024. Front Oncol. 2024. PMID: 39239275 Free PMC article. Review.
-
Hepatocellular Carcinoma Patients with Hepatitis B Virus Infection Exhibited Favorable Survival from Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis.Liver Cancer. 2023 Oct 30;13(4):344-354. doi: 10.1159/000534446. eCollection 2024 Aug. Liver Cancer. 2023. PMID: 39021889 Free PMC article.
-
Case report: The efficacy of adding high doses of intravenous vitamin C to the combination therapy of atezolizumab and bevacizumab in unresectable HCC.Front Med (Lausanne). 2024 Oct 3;11:1461127. doi: 10.3389/fmed.2024.1461127. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39421875 Free PMC article.
-
A novel super-enhancer-related risk model for predicting prognosis and guiding personalized treatment in hepatocellular carcinoma.BMC Cancer. 2024 Sep 2;24(1):1087. doi: 10.1186/s12885-024-12874-7. BMC Cancer. 2024. PMID: 39223584 Free PMC article.
References
-
- Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers 2021;7:6. - PubMed
-
- Villanueva A Hepatocellular carcinoma. N Engl J Med 2019;380:1450–1462. - PubMed
-
- Galle PR, Forner A, Llovet JM, et al. EASL Clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2018;69:182–236. - PubMed
-
- Marrero JA, Kulik LM, Finn RS, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 2018; 67:358–380. - PubMed
-
- Llovet JM, Bruix J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology 2003; 37:429–442. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
